What was at one time called PLUG, and, with the change from open to endoscopic intervention, is now called FETO (fetal endoscopic tracheal occlusion) is a way to harness the normal physiology of the lung in congential diaphragmatic hernia (CDH) to improve lung growth and architecture in order to improve outcomes. Lung growth is partially dependent on the rhythmic increases in fetal intrapulmonary pressures which occur because of the active production of fetal lung liquid and intermittent breathing movements of the fetus associated with partial adduction of the vocal cords. Numerous fetal animal studies showed that interrupting this process (with phrenic nerve section or tracheotomy, for example) leads to pulmonary hypoplasia, while increasing the intrapulmonary pressures, by ligating the trachea, caused pulmonary hyperplasia. Finally animal models of diaphragmatic hernia followed by tracheal obstruction showed at least partial normalisation of lung growth. Interventional obstetricians and paediatric surgeons have attempted to temporarily obstruct the fetal trachea in some fetuses with CDH and very high predicted mortality. Initial attempts were apparently successful, but with a risk of preterm labour and delivery.
The improvements in technique and change to purely endoscopic approaches have led to lower complication rates (importantly prematurity), but it remained unclear whether, overall, survival was improved.
The recent publication of the results of 2 parallel trials in high-risk and moderate-risk patients has largely answered that question.
Deprest JA, et al. Randomized Trial of Fetal Surgery for Severe Left Diaphragmatic Hernia. N Engl J Med. 2021.
Deprest JA, et al. Randomized Trial of Fetal Surgery for Moderate Left Diaphragmatic Hernia. N Engl J Med. 2021.
This was a remarkable undertaking, a truly international collboration in a group of mothers carrying a fetus at extremely high risk of dying. And here, as an aside, I always feel a little uncomfortable with the way we talk about these interventions. Although it was indeed “fetal” surgery, there happens to be a woman in the way! Perhaps we should rather talk about “maternal-fetal” interventions. Even the pretty pictures below represent the mother just as an abdominal and uterine wall to be pierced…

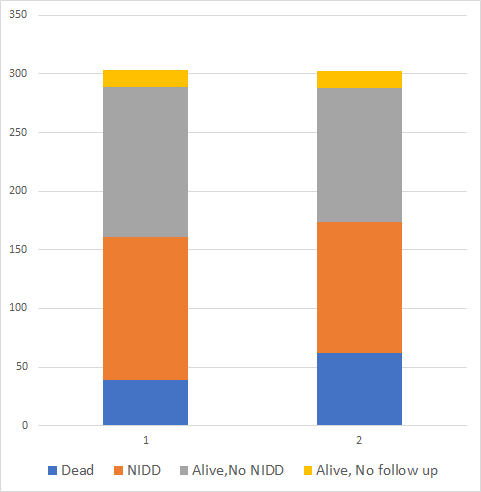
As you can see from this summary, there was a dramatic improvement in survival. I do think it is important to emphasize that there is still a very high mortality of 60% in the treatment group; this is a terribly high risk group of babies. The eligibility criteria included a ratio of observed to expected lung-head ratio (O:E LHR) of less than 25%, predicting a mortality of about 82%, very close to the 85% actually seen in ther controls. The median age of delivery for the FETO babies was 34.6 weeks compared to 38.4 for the controls; this doesn’t sound like a huge difference, but 16 FETO babies delivered before 34 weeks compared to 0 controls, and 10 of them delivered before 32 weeks. Managing moderately preterm babies with CDH is very difficult. It seems likely that if we can find ways to prevent the rupture of membranes and preterm labour impacts of FETO, the benefits would be even greater.
The other trial was run in parallel, it enrolled mothers carrying a fetus with an observed lung to head ratio that was 25.0 to 34.9% of the expected, irrespective of liver position, or 35.0 to 44.9% with intrathoracic liver herniation. This was calculated to lead to a survival of 55% and sample size calculated for a 20% improvement.
The primary outcome was actually changed early on by the DSMC of the trial, which was initially designed with a primary outcome of BPD, or oxygen dependence at 28 days, with survival to discharge as a secondary outcome. I think the DSMC did exactly the right thing here, I don’t know who thought that 28 day oxygen requirement was important for infants with CDH, but to have given that priority over survival would have been a major problem. Perhaps that was initially chosen as the investigators are Obstetricians, not Neonatologists (he typed with tongue in cheek)?
Survival to discharge was higher in the FETO group, 62 of 98 treated compared to 49 of 98 controls, RR 1.27 (95%CI 0.99-1.63), as the confidence intervals for the RR just includes 1.0 the intervention was deemed not to show a significant benefit.
The impact on prematurity was very similar to the high-risk group trial, with the median gestational age at delivery being 2 weeks earlier with FETO than control, but both groups being about 2 weeks later than the other trial, that is 36 weeks for the FETO and 38 weeks for the controls. The relative risk and risk difference of being born before 37 weeks was very similar in the 2 studies.
Although this was a “moderate” risk trial, there was still a huge mortality of 50% in the controls (showing again that the O:E LHR is a reliable predictor of mortality), 20% of both groups required ECMO, and they had between 1 and 3 months of hospitalisation (average about 48 days in each group).
The division into “severe” and “moderate” risk groups (perhaps better termed “extreme” and “severe”) was completely arbitrary. A threshold of 25% O:E LHR could easily have been set to 30, or 31.5%. Such a threshold would have included more infants in the extreme trial, and I can guess would not have changed the result to a “non-significant” result.
In fact I don’t have to guess, because if these trials had been run as a single trial and included all the babies eligible for the two trials, with subgroups of extreme and severe risk, then the total survival to hospital discharge would have been 78 of 138 FETO babies and 55 of 138 controls; p=0.0081 (chi-square with Yates correction). In that case the conclusion would have been that FETO is beneficial for babies with an O:E LHR of < 35%, and for babies with intrathoracic liver with an O:E LHR of <45%, perhaps with a subgroup analysis showing a greater effect in the most severely affected fetuses.
It is evident that, at some point, the increased relative risk of prematurity (which was similar between the trials) will outweigh the benefit of the procedure, but we cannot from these data conclude that below a threshold of 25% O:E LHR, FETO is overall a beneficial intervention, but that above 25% it is not beneficial. Unfortunately, I think that is how the data will be interpreted. A secondary analysis of the overall survival benefits of FETO according to baseline O:E LHR needs to be performed, otherwise mothers carrying fetuses who would benefit will not be offered the intervention.
There are not many conditions in medicine for which a trial of 80 patients will show a dramatic and reliable difference in outcome between groups. The substantial benefits of this intervention for a profoundly serious condition mandate that all centres that have potential links to an experienced FETO centre should find a way to offer the intervention to mothers carrying an eligible fetus.
Currently, mothers who have had the procedue need to stay within reach of the FETO centre until the balloon is removed, for very good reasons. This creates limitations for many families, which may be insuperable, our FETO centre for example is 550 km away, for some mothers for other parts of the province it will be 2000 km away! Moving to live in Toronto for 8 weeks is not necessarily feasible for some mothers, especially as health care costs are all covered by our provinicial systems, but not daily living expenses. I wonder if we could create satellite centres who would develop the expertise required to remove or puncture the balloon in case of preterm labour, or routinely at 34 weeks, including the team, the equipment, and the protocols. Then a mother could travel to the FETO centre for the procedure, stay a couple of weeks in the region, and then return to be close to a satellite centre for the rest of the pregnancy. I have no relevant expertise in the interventions, but it seems to me that ultrasound guided balloon puncture is not that different to many of the interventions performed by our MFM specialists, at least compared to fetal bronchoscopy which seems to me to be a greater level of complexity.
Thank you to the mothers who were prepared to be randomised in this trial, which will have a major impact for many future babies. Your willingness to help others is enormously appreciated.