I mentioned not so long ago that the web page of the US Obstetricians professional association has information for prospective parents of babies of less than 25 weeks gestation that is… questionable.
They state, for example, the following :
Medical advances have helped some preterm babies survive and overcome health challenges. However, the chances that a baby born extremely early will survive without disability are still small. With very rare exceptions, babies born before 23 weeks of pregnancy do not survive. Although survival rates increase for babies born between 23 weeks and 25 weeks of pregnancy, most survivors face serious, often lifelong disabilities. As gestational age increases, the outlook for preterm babies improves.
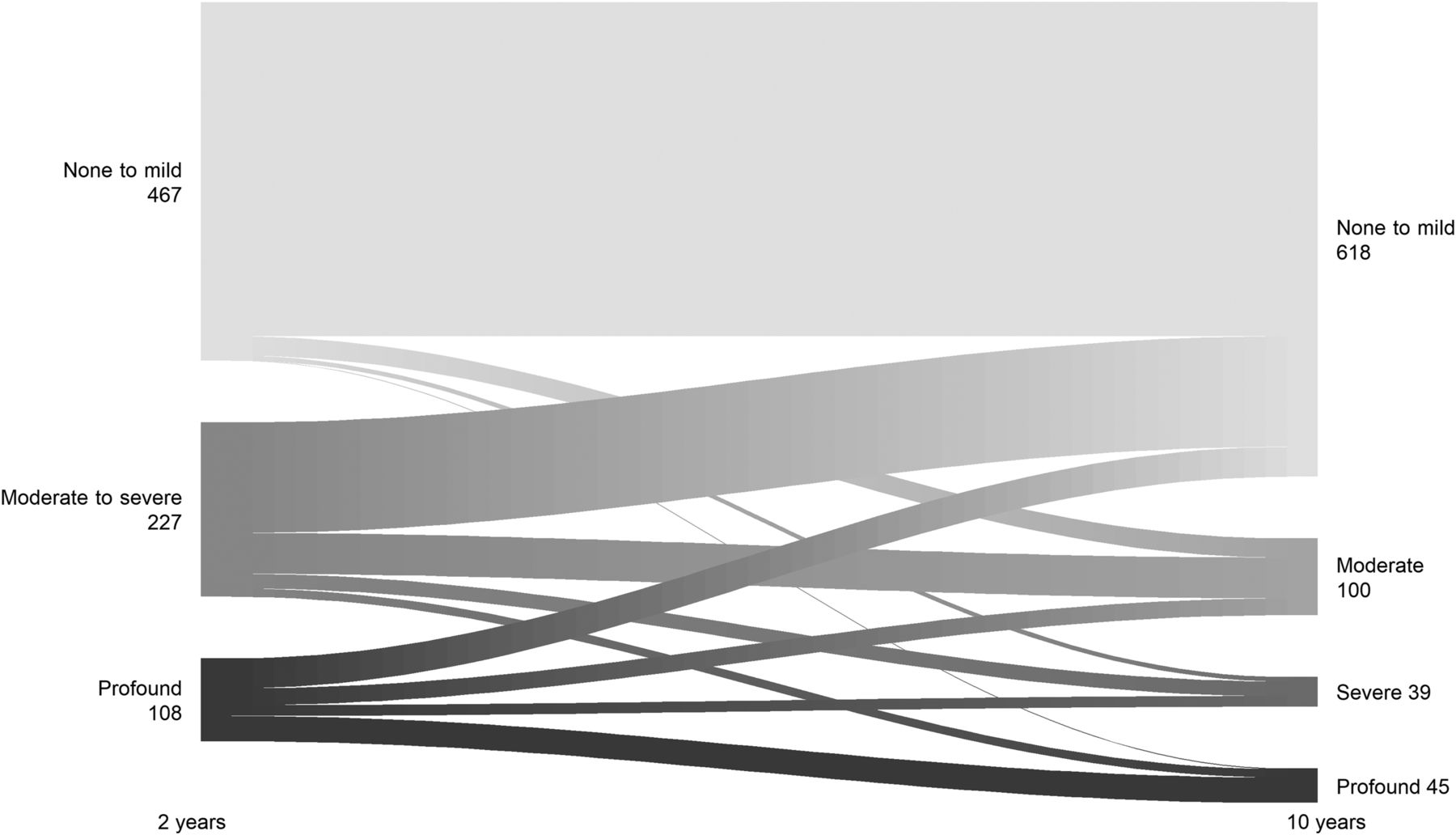
That statement is wrong factually: in Japan, with the majority of babies at 22 weeks receiving active intensive care, 50% of them survived in 2010, similar results from Uppsala can be seen with 53% surviving over a 10 year period, 2006-2016. In Iowa over a 10 year period survival at 22 weeks was 64% among babies receiving active intervention (almost all the live births), similar to the data from Cologne. A systematic review of the available data for babies of 22 weeks GA showed that infants receiving “proactive” treatment had an overall survival among published cohorts of 29%; survival was better in the later epoch (2010-2020) at 31% compared to studies from before 2010, 22%. I don’t know what ACOG thinks of as “very rare exceptions” but 1 in 3 babies surviving is hardly very rare. Similarly the statement: “most survivors face serious, often lifelong, disabilities” is factually incorrect. Most survivors have no disability or mild disabilities (for example 70% of survivors in Uppsala, 55% in Iowa), and, as most “disability” is because of low scores on Bayley testing, the proportion with disabilities decreases with time.
Why our Obstetrical Colleagues are so biased against the most immature babies confuses me. You would think that they would be our greatest allies in trying to improve outcomes for the patients we have in common, that they would want to help mothers and their partners to make the best decisions based on accurate information.
What would unbiased information actually look like? I think it should include the following information which is critically important to parents facing the challenge of a potential delivery at <25 weeks.
1. Determination of the exact gestational age is inexact. Remember that if you have an assigned gestational age of 23 weeks and 1 day, for example, you might be at 22 weeks and 3 days or at 23 weeks and 6 days.
2. Threatened extremely preterm delivery often calms down, and many mothers deliver at less frightening gestations.
3. Many factors affect your babies chances if delivery actually happens, more than just the number of weeks: the weight of the baby, whether it is a boy or a girl, a single baby or one of twins, presence of infections, whether you had a chance to get a steroid injection, where you actually deliver the baby. All of these can make a difference between having a very small chance of survival and having a much better chance.
4. In some hospitals babies under 24 weeks, and in others under 23 weeks, are not offered intensive care. Other hospitals have a much more proactive approach. Ask your obstetrician if your hospital has any policies, and any experience, in giving intensive care support to babies at your estimated gestational age.
5. Before 22 weeks best estimate of gestational age there are only very few babies in the whole world who have survived. After 22 weeks estimated gestational age chances improve, and continue to improve with each day. Overall, in a hospital that gives babies at 22 weeks GA a chance, 1 out of 4, to as many as 1 out of 2, babies can survive.
6. Almost always, babies at 22 to 23 weeks gestational age have several complications during their hospital stay, they tend to have infections, feeding problems, lung development problems and many have serious complications.
7. If your baby survives the first 24 -72 hours their chances will improve. Most babies who don’t make it die within that period. However, some who have multiple or very serious complications can get into serious difficulties later and may die after many weeks of intensive care.
8. Babies who survive frequently have challenges during their first years, many have lung problems and hospital visits, or re-admissions, often for lung problems. Some will need surgery, such as for a hernia. Some will need extra attention from physiotherapists, occupational therapy specialists, and other medical specialists. Almost all have an excellent quality of life, are able to communicate, and enrich the families they are born into.
As I was preparing this post, a highly relevant review article by John Lantos was published (Lantos JD. Ethical issues in treatment of babies born at 22 weeks of gestation. Arch Dis Child. 2021) John points out how strange the response has been to the incredible successes in looking after the most immature babies:
One might expect that such a startling medical breakthrough would stimulate excitement, admiration, emulation and research. Oddly, it seems to have generated none of those things. Instead, key professional societies have either ignored or misrepresented the outcome data.
He suggests that what is holding us back is inertia “Treatment of babies born at 22 weeks of gestation shows very promising results. Parents seem to want such treatment. It is cost-effective. The reticence of many centres to provide such treatment seems to be a result of institutional inertia.”
I am not so sure that is all it is, the bias of obstetrical groups against these babies is strong. I wonder if it is because they sometimes perform terminations at 22 weeks for babies without congenital anomalies, so they would rather believe that they are non-viable. There is also an extremely negative sentiment regarding cesarean delivery at extremely low gestational ages, but I think that the decision to be proactive with care does not mandate that a cesarean delivery be performed. Some centers with good results (like Uppsala) have zero CS at 22 weeks, others do some caesareans. Iowa also reports no C-Sections at 22 weeks, but over 1/3 at 23 weeks. I think like everything else it should be an individualized decision, taking into account, among other things, the mother’s future reproductive plans. A mother who is 40 years old with previous pregnancy losses, and a 20 year old in her first pregnancy will probably have a different balance of risks and benefits.
I do believe that my obstetrical colleagues are working for what they think are the best interests of their patients, and I also think that active intervention at 22 weeks should be a shared decision with the mothers. But, in order to make that shared decision, mothers, and their partners, need accurate information, with realistic predictions of what will be the result of insituting NICU care. The current ACOG website, last reviewed in August 2019, is full of inaccurate information, that was incorrect in 2019, and even more so today.