
In this post, I continue to discuss some of the issues raised in our recent article: Chevallier M, Barrington KJ et al. Decision-making for extremely preterm infants with severe hemorrhages on head ultrasound: Science, values, and communication skills. Semin Fetal Neonatal Med. 2023:101444. My musings here are not identical to what you will find in that article, which I encourage you to obtain and read.
When it comes to more severe abnormalities. it remains the case that the prevalence of major disability correlates poorly with the Papile grade of IVH. This is in part because of some diagnostic ambiguity; some grade 2 hemorrhages are followed by early ventricular dilatation and may be reclassifed as grade 3 hemorrhages. In addition grade 3 hemorrhages are usually lumped with grade 4 hemorrhages in follow up studies, and it is thus not clear if their prognosis is better or worse, or similar. Also, grade 4 hemorrhages vary enormously from small localised intracerebral bleeds to massive bilateral hemorrhage.
There are a couple of published severity grading systems, the Bassan and Al-abdi systems, which have been evaluated in independent cohorts. Both show that there are smaller grade 4, or intraparenchymal, hemorrhages which have very little effect on outcomes. As IPH becomes more extensive the range of outcomes tends to shift to more cerebral palsy, and greater impacts on development. Even the most severe IPH are by no means universally followed by profoundly impaired futures.
A huge limitation of this field is that outcomes are usually defined by performance on standardized testing of developmental status, usually at 18 months to 2 years of age, and not by the impacts on function. I am very uncomfortable with the idea of taking a potentially life-shortening decision based on the probability that an infant may have a low BSID score.
A better way of thinking about how impairments impact patients and their families, that I find very insightful, is to think about the F-words. (Rosenbaum P, Gorter JW. The ‘F-words’ in childhood disability: I swear this is how we should think! Child Care Health Dev. 2012;38(4):457-63). The F-words refer to important features in the lives of children with all types of disabilities.
Function, Family, Fitness, Fun, Friends and Future.
They are interrelated, of course, as this diagram from that publication tries to illustrate

Of Note: this brilliant article is open access, please download, read, and distribute!
Function is a broad term referring not just to impairments, but to capacity and performance, which are related but distinct concepts, for example, even with limited capacity for certain tasks, the performance of an individual can be improved by practice and exercise.
In our recent article, about the outcomes of children who survived after end-of-life decisions, we used a functional outcome scale to describe how the children were doing, which I think is much more useful than scores on developmental screens, or even on IQ tests, when we are discussing values and quality of life. That system, the Glascow Outcomes Scale-Extended (GOS-E) has the following grades : GOS-E of 1 is a “normal” functional outcome, 2 is “normal” function with ongoing medical needs, 3 is permanent impairment, but with a prospect of independent living, 4 is disability with likely supervised living in the future, 5 is disability requiring assistance with activities of daily living, 6 is disability requiring assistance with activities of daily living needing the permanent presence of another person, 7 is complete dependence on another individual with no possible communication, 8 is death.
As mentioned, I don’t think that Bayley scores (or IQ results) are relevant for decision-making for whether or not we should continue life-sustaining treatments or not. Functional outcomes are much more important, and the little data available suggest that the general public agree with that. In an interesting study questioning adults on-line, Dominic Wilkinson and his group described several scenarios, all based on recent high-profile legal cases in the UK, and they asked the respondents whether they thought life was of value for the infant, and whether withdrawal of intensive care was permissible. Most of the respondents in the UK agreed that, for an infant with no awareness of their surroundings, or with only “possible” awareness, life was of little or no value, and that withdrawal of care was either permissible or mandatory.
The following was one of their cases, a child with profound limitations,

The large majority of respondents thought the this child’s life was of benefit to them, and 75% thought that continuing intensive care was morally obligatory. Only 12% stated that if it were their child they would want treatment withdrawn.
Such profoundly limited function, equivalent probably to a GOS-E 6 or worse, is very rare in our preterm population, with or without intracranial bleeds. But it is impossible to find any literature correlating severity of early ultrasound abnormalities with a functional outcome evaluation that is really relevant to decision making.
What we are, therefore, currently faced with, is trying to predict whether outcomes will be so poor that continuing intensive care is questionable, and is something to be discussed, but based largely on guesswork, and on the risks that a baby will have “NDI”, but even “severe NDI” is far from what the general public think is a good reason for withdrawing Life-Sustaining Interventions.
If we display data such as that from Radic et al, the outcomes of their grade 4 group, if they were normally distributed, the developmental screening test scores would look like the orange curve below. The majority of the babies are to the right of the 70 line, and therefore not “severely impaired”

We could display the data from that study in arbitrary categories of severity, which follow-up studies are very keen on doing, in which case they would look like this:
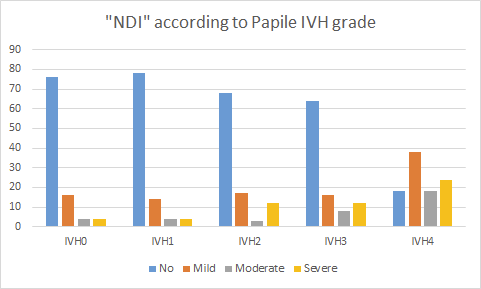
These are the results (Radic et al) from the surviving babies who had follow up, which I estimated from the figure in the publication. Severe NDI in that study was severe CP [severely impaired ambulation or nonambulatory] and/ or developmental scores > 3 SD below the mean, and/or bilateral blindness.
As you can see, few babies with grade 3 bleeds have the “worst” grade of outcomes, less than 15%, and only 24% of those with grade 4 bleeds had “severe disability”. I can’t help but state this again, a low score on a developmental screening test is NOT a disability, or an impairment! Some children with such low scores will indeed eventually prove to have a “loss of function” which is an abbreviated definition of an impairment, and in some cases this might lead to a “limitation in activity or participation” an abbreviated definition of disability. But many will not.
That graph shows, yet again, that a serious abnormal finding on an early head ultrasound, shifts the uncertainty, at least regarding probable future developmental screening test results, but there will always be a large range of possible outcomes for an individual.
Here are similar data, just for the most severe IVH, from Desai et al

Again, only a minority (25%) of infants with a history of IPH (or IVH4) had “severe NDI” defined as cognitive scores of >3 SDs below the mean, GMFCS level IV/V CP, and blindness (vision, <6/60). Cognitive scores in this study were either Griffiths or BSID2 or BSID3.
The rare baby who is so profoundly affected that the general population would consider it reasonable to consider limitation of Life Sustaining Therapies, is probably in a subgroup of the “severe NDI” category. The proportion of babies with an IPH who have outcomes that are so severely impaired will therefore be rather less than 20%. Can we figure out which babies with IPH might end up with such poor outcomes?
Are more extensive IPH better for predicting severely abnormal outcomes? Both the ELGAN cohort, and the study by Nathalie Maitre have shown that bilateral IPH is a better predictor of CP than unilateral IPH, but not all of which was severely disabling CP. Two other studies found very poor association between Bassan scores of the severity of IPH and developmental scoring at 2 years, the Al-Abdi score seems slightly better correlated with developmental scores than Papile categories, but the differences are minor. There doesn’t seem to be any good data relating IPH severity to longer term intellectual outcomes, nor to important functional abilities.
Our problem, then, is not just the uncertainty inherent in trying to predict the future for an individual, (the kind of problem that many physicians, such as oncologists and surgeons, are often faced with), but a serious lack of relevant information. How often does a particular head ultrasound abnormality (such as an extensive unilateral IPH, for example) actually lead to serious functional limitations, with an impact on abilities to communicate? I don’t know, indeed no-one does.
I think it is really important to remember the following:
- most babies with “NDI” are classified as such because of low scores on the BSID (or other developmental screening test)
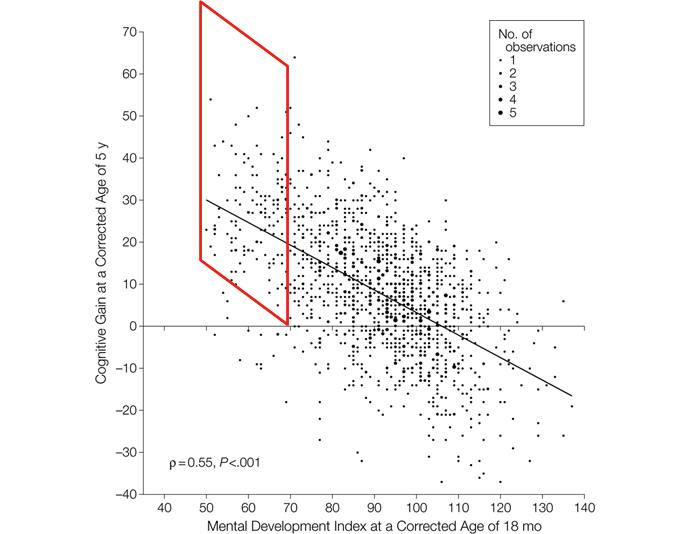
- most babies with low BSID scores at 2 years do not have life-changing impairments, they don’t even have scores on IQ tests which are low if you retest them at 5 years, if you look at the figure below taken from the 5 year follow up of the CAP trial, you can see that most babies with “severe DI” that is a Bayley MDI >2SD below the mean, had an IQ on the WPPSI-3 above 70 (all those with dots within the red parallelogram).
3. Most babies with low BSID scores function very well, and have a normal quality of life.
I don’t mean to suggest that having a low score on an IQ test is a sign of a serious impairment warranting limiting LST! It is just one illustration of the limited value of early developmental screening tests for the long term.
Finally, all that we can really say for more serious abnormalities on early head ultrasound is that they shift the uncertainty a little bit more than minor abnormalities. Developmental progress is pushed more to the left, and more babies fall into arbitrary categories of moderate or severe delay.
What those categories mean to parents will be the subject of the next post…. coming soon.







Pingback: What outcomes matter to parents? | Neonatal Research
Pingback: Comprendre les saignements cérébraux chez les prématurés : Une analyse de la littérature médicale et des pratiques cliniques – Dr Annie Janvier
Pingback: Understanding cerebral bleeding in preterm infants: An analysis of medical literature and clinical practices. – Dr Annie Janvier