
Routine early head ultrasound is the de facto standard of care in preterm infants. Recent statements from learned societies usually recommend head ultrasound at around 7 days of age, and many centres do them earlier than that.
Older statements suggested that the reason for early routine ultrasound was to decide about the appropriateness of continuing intensive care, more recently they tend to suggest their importance for finding treatable abnormalities, such as IVH with an increased risk of post-hemorrhagic hydrocephalus, and for predicting outcomes.
In a new publication we tried to summarize the data about prognosis of serious abnormalities on early head ultrasound, and then provide some guidance about how to discuss findings with the parents. Chevallier M, Barrington KJ et al. Decision-making for extremely preterm infants with severe hemorrhages on head ultrasound: Science, values, and communication skills. Seminars in Fetal and Neonatal Medicine. 2023.
When we look at the entire literature which has examined associations between abnormalities on brain imaging (ultrasound or MRI), we find very little information that we can use to talk to parents about the implications for their individual baby. Most studies have investigated, and shown, some sort of overall group correlation between worse imaging findings and poorer outcome. For example, with large enough datasets, one can show that there is a statistically significantly worse outcome among babies with a grade 1 or grade 2 hemorrhage compared to babies without hemorrhage.
I submit that this information is of extremely limited value for counselling individual parents. Here is the Forest plot from a recent meta-analysis of the impacts of grade 1 and grade 2 hemorrhages (which is to say hemorrhages confined to the sub-ependymal region and/or blood within, but not distending, the ventricles)

The plot shows the adjusted Odds Ratios for having what is labelled “moderate-severe NDI” is probably about 1.35. Which looks really bad.
Perhaps we should tell parents after the ultrasound: “your baby had a grade 2 IVH, she now has a 35% greater odds of having a moderate to severe handicap than if she did not have the IVH”…. Or Perhaps Not.

The prevalence of what is called “moderate-severe NDI” is 20% with a grade 1 to 2 hemorrhage, and 17% without a hemorrhage, if we add all these studies together. Of note the data from Bolisetty which are used in this graphic and analysis are actually the data for “isolated” grade 1 and 2 IVH, which is those which were not followed by PVL, porencephaly, or ventricular dilatation. That eliminated 40 of their 336 grade 1 and 2 IVH. Other studies have used the worst head ultrasound findings, or have not stated if they eliminated some of the cases post-hoc if they developed other brain injuries. The data from Sharkaran et al actually include all grades of IVH that did not develop post-hemorrhagic hydrocephalus, therefore including some grade 3 and 4 hemorrhages, rather than just grades 1 and 2.
Perhaps we should tell parents after the ultrasound: “your baby had a grade 2 IVH, her relative risk of having a moderate to severe handicap is 18% higher than if she did not have the IVH”…. Or Perhaps Not.
The majority of so-called “Moderate-Severe NDI” is low scores on developmental screening tests, which, in the studies in these Forest plots, was either Bayley Scales of Infant Development version 2, or version 3 or Griffiths, or, in some studies, both BSID 2 and 3 were used depending on the year. Ages of follow up were from 18 months to 3 years. The specific items which led to a classification of “Moderate-Severe NDI” were either BSID2 MDI <70, or BSID3 cognitive score of <70, or either scale of the BSID 2 <70, or either motor or cognitive score on the BSID3 <70, or a mixture.
So perhaps we should tell parents after the ultrasound: “your baby had a grade 2 IVH, her relative risk of having a low score on the developmental screening test is 18% higher than if she did not have the IVH”… Or Perhaps Not.
Or, as mentioned below, people generally understand absolute risks better than relative risks. A more appropriate way of talking about the impact of a low grade IVH could be “there is a chance of the babies developmental assessment at 18 months to 3 years giving a low score; having the grade 2 IVH increases this chance slightly, from 17 babies out of every 100 having a low score to 20 out of every 100”.
Let us try and think about what that means for the population, and for an individual.
The average BSID MDI score was about 97 for very preterm infants (<30 weeks) in the study included in the above systematic review from Nova Scotia (Radic et al) who did not have an IVH, and, if they are normally distributed, this gives the distribution of scores shown below as the blue line.
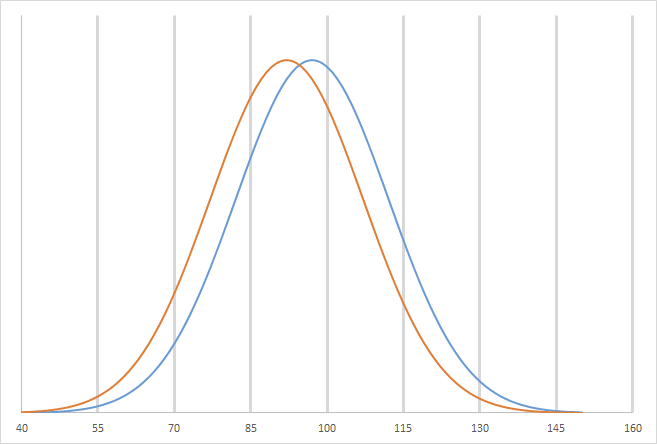
The babies with grade 2 hemorrhages have BSID scores shifted downward, according to the results of that study, to a mean of around 92, (but the infants were also less mature and smaller with more other complications), which gives the orange line. As a result the proportion of babies with scores < 70 increases, in that study from about 20 to 26%, for grade 2 IVH.
One could ask if the scores among former preterm babies are indeed normally distributed, and they probably are, with perhaps, in some cohorts, a slight skew at the bottom end. It is very hard to be sure, however, as the data are not usually given; even when the mean and SD of the scores are described, the actual distribution is very rarely shown. It is something which we did show in the report of the 2 year outcomes of the CAP trial, which showed a shift upwards of about 3 points of the mean BSID2 MDI score in the caffeine group compared to the controls. Below is the graph of the cumulative distribution of the scores. You can see, at the bottom of the curves, that they are truncated at 49, as the few untestable babies were all assigned a score of 49.

It certainly looks very similar to a graph of the normal distribution displayed in a similar cumulative fashion, such as the one below with a mean of 0 and and SD of 1.

The point I am trying to make, starting with the example of low grade IVH, is that the head ultrasound result just shifts the uncertainty a little. In a stable preterm baby with no other medical complications, having a grade 1 or 2 IVH does, probably, overall, have a minor impact on developmental progress in early infancy, if we examine a large number of babies.
What does that mean for the individual baby in their mother’s arms? How should we explain to parents, of differing educational and social backgrounds that the outcome of their baby is just as uncertain as it was before the head ultrasound, but the risk of having developmental delay is slightly greater, that the zone of uncertainty has been shifted downwards, a bit? Do most of us even understand risk?
Of course we are not alone, many other physicians and counsellors have to talk to their patients (or parents) about risks of long term outcomes. Usually, I think, they are talking about things which are not quite as nebulous as scores on developmental screening tests, rather they try to discuss prognosis for survival, recurrence, colostomy, amputation, etc. even then there is always uncertainty, and almost never an ability to state with confidence what will happen to the individual.
Parents “often lack the health literacy needed to understand the words that their doctors use when describing medical alternatives. Patients even have difficulty comprehending many of the educational materials they receive from health providers. Although an average American reads at eighth grade reading level, health education materials are often written at a high school or college reading level, making the information contained in them inaccessible to the targeted audience.
Second, many patients have low numeracy skills, leaving them less able to derive useful meaning from the numerical information often presented in such materials (eg, risk and benefit statistics). To put the issues of low numeracy into perspective, approximately half of the adults in the United States are unable to accurately calculate a tip, and 20% of college-educated adults do not know what is a higher risk—1%, 5%, or 10%. Thus, when an oncologist tells a patient that his or her 5-year chance of survival is 85% or if an educational pamphlet informs patients that the risk of nausea from chemotherapy is 55%, many patients will not understand such statistics well enough to use them as part of making an informed decision.
Fagerlin A, et al. Helping patients decide: ten steps to better risk communication. J Natl Cancer Inst. 2011;103(19):1436-43.
That article from Peter Ubel and colleagues has 10 recommendations, based on the literature on decision-making and patients’ understandings of risks.
- Use plain language to make written and verbal materials more understandable.
- Present data using absolute risks.
- Present information in pictographs if you are going to include graphs.
- Present data using frequencies.
- Use an incremental risk format to highlight how treatment changes risks from preexisting baseline levels.
- Be aware that the order in which risks and benefits are presented can affect risk perceptions.
- Consider using summary tables that include all of the risks and benefits for each treatment option.
- Recognize that comparative risk information (eg, what the average person’s risk is) is persuasive and not just informative.
- Consider presenting only the information that is most critical to the patients’ decision making, even at the expense of completeness.
- Repeatedly draw patients’ attention to the time interval over which a risk occurs.
I wonder how many of us really understand what “an adjusted Odds Ratio of 1.35 of moderate-severe NDI” really means. I don’t suppose any of us would actually use those words when talking to parents, but can you explain that in clear language, that someone reading at an eighth grade level (about 13 years of age for the non-Americans) would understand? If you can do so, then 50% of your parents would still not understand! (And half of them would not even know what 50% means!) It is not, of course, just understanding the words or the numbers, but the subtle concepts underlying uncertainty, and trying to comprehend what that might mean for one particular baby.
Perhaps my usual approach for a baby with a grade 1 or 2 IVH, is reasonable after all, of just telling the parents, “the small bleed we just saw has almost no impact on your baby’s long term prospects, (s)he will almost certainly function well and have a good quality of life” which is a phrase you can say for almost all our babies. What about more serious brain injury? Part 2 is coming…






