As frequent readers of the blog will know, there are major concerns about using the classical dichotomous composite outcomes for trials. One of the outcomes included is usually death, as it “competes” with many other outcomes, and the other components in the composite may range from the extremely important such as ‘NEC requiring surgery’ or ‘profound disability’ to the less important, such as culture-negative sepsis, or oxygen requirement at 36 weeks.
A dichotomous composite outcome treats all components as if they are equal; adding components to the outcome may increase the power (although not always) especially when some of the outcomes are rare. So studies investigating therapies in infants of 28 to 32 weeks will need to be enormous to show differences in mortality, as it is relatively uncommon, but if a second outcome of higher incidence is added, such as failure to extubate by 12 hours as an example, sample size may become manageable. Thus trials with multiple components of the primary outcome have been developed, sometimes being rather unwieldy. For example, the recent LIFT trial of lactoferrin prophylaxis (Tarnow-Mordi WO, et al. The effect of lactoferrin supplementation on death or major morbidity in very low birthweight infants (LIFT): a multicentre, double-blind, randomised controlled trial. The Lancet Child & Adolescent Health. 2020;4(6):444–54) used the following as its composite primary outcome “death or major morbidity, defined as: brain injury on ultrasound, NEC, (Bell stage ≥II), culture-proven late-onset sepsis, or RoP requiring treatment”. The now completed LIFT_Canada trial was designed to be identical to LIFT in order to be able to perform an IPD analysis, so we used the same composite outcome (Asztalos EV, et al. Lactoferrin infant feeding trial_Canada (LIFT_Canada): protocol for a randomized trial of adding lactoferrin to feeds of very-low-birth-weight preterm infants. BMC Pediatr. 2020;20(1):40). Other trials have had even more components to the outcome, which can make interpretation difficult, but might also actually decrease power, as large proportions of subjects will have at least one of the outcomes, and be counted as an adverse result, which might hide real important differences.
Among the problems with dichotomous composite outcomes are that if different parts of the composite change in different directions, then the overall analysis may be null, which might hide an important benefit, or adverse effect. The best example of this in neonatology is the SUPPORT trial, which showed a reduction in RoP (which was expected) but an increase in mortality (which was a surprise, but has been confirmed by other trials), when babies received oxygen targeting a lower saturation of 85-90% rather than a higher 91-95%. The primary outcome was not different between groups, even though most people would agree that dying is a worse outcome than “threshold retinopathy or retinal surgery or bevacizumab injection” (the definition of severe RoP used).
One way to address these problems is to use Hierarchical Composites, where the various parts of the composite are placed in ascending order of seriousness. The analysis requires either that the patients are entered as pairs, and each is compared to the paired patient in the other group, or, now more commonly, every individual in group 1 is compared to every individual in group 2. For each paired comparison, if one survives and the other dies then the survivor is declared the winner. If both die, then the outcome is a draw. If they both survive, then the second outcome in severity is compared, and a winner (if there is one) is then declared, and so on through the list of outcomes of diminishing importance. Eventually a winner or a draw is determined.
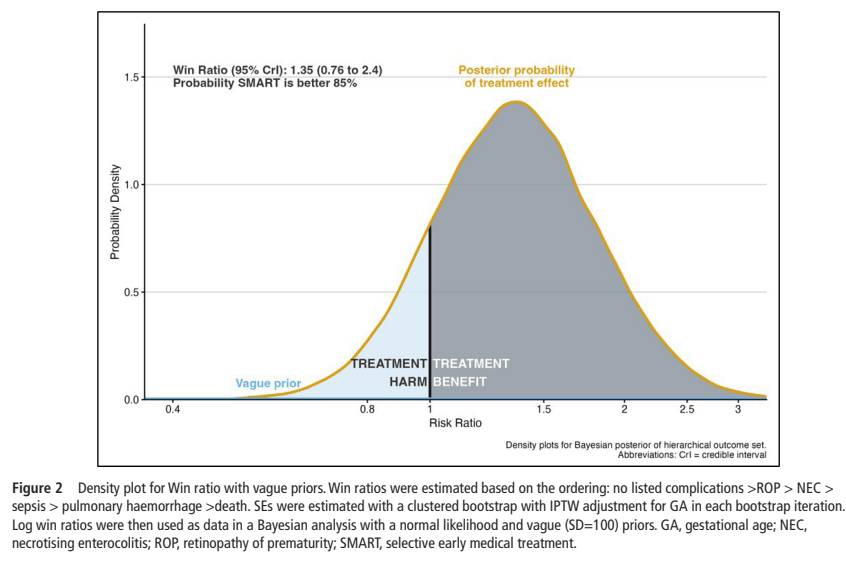
The analysis of such outcomes is still being developed, the simplest, I think, is the “win ratio” (Cunningham JM, et al. Win Ratio Method for Hierarchical Composite Outcomes in Randomized Clinical Trials. JAMA. 2026) that I have written about a few times. There are several examples of trials where the primary analysis of the outcome as being dichotomous has shown a null result, but the analysis using win ratio has been significant, demonstrating a real clinically important difference in the results between 2 interventions, missed by conventional methods. Several trials have more recently been designed to primarily use Win Ratio, or other hierarchical endpoint analyses.
That article by Cunningham discusses the analysis of a recent cardiovascular therapy trial (where these types of endpoints have been most widely used), and points out that the significant difference between results that the trial found (comparing 2 different treatments in Chagas’ disease cardiomyopathy) was not in mortality, or hospitalisation, as you can see from the figure below, but in the results of a blood test, measuring the change in NT-proBNP. The figure shows the number of wins for each group, the number of ties, and the overall difference between groups, which was almost entirely due to changes in the serum marker.

This points out a limitation of this kind of trial analysis, it is important to include items which are of clinical significance, that is, they are of significance to patients. I doubt that many people care too much about the relative changes in their NT-proBNP. Perhaps how far they could walk without being breathless, or something else of importance to the patient, should have been measured.
Indeed, how the components of the composite are chosen and their relative importance is a major question for future trials. As another article in JAMA points out (Ehrenzeller S, et al. Randomized Clinical Trials Using a Hierarchical Composite Primary End Point: A Scoping Review. JAMA Netw Open. 92026. p. e2625935), of the 92 trials they found which had used hierarchical composites, the large majority, 82%, included no information about how the hierarchy was developed.
It is essential that multiple different stakeholders are involved in developing future hierarchical composites, and that, importantly, parents and former sick newborns are given a free voice in suggesting their own priorities. (Callahan KP, et al. Integrating parent voices into research at the extremes of prematurity: what are we doing and where should we go? J Perinatol. 2024). Much as I admire the development of Core Outcomes Lists, often the processes involved have had parents and other partners choosing among our predefined list of possible outcomes. The parents voices project, though, has shown that some of the things that we include in lists of outcomes are of little importance to parents (Demers C, et al. Measuring family-important outcomes in large neonatal networks: where we are and where we need to go. Semin Perinatol. 2025;49(7):152149), such as needing oxygen at 36 weeks (!), and others that we rarely discuss, and don’t even measure (such as feeding problems post-discharge), are very important to them.