
After my recent post, about the study which suggested that donor milk was killing babies, I have been taking a deeper dive into the article, as I prepare a letter to the editor.
Only 2 small subsets of the infants in the database were analyzed, of the 36000 babies in the database, 1000 received only MBM and DHM, and never received any fortifier or formula from the day of birth until death or discharge. They had an enormously high mortality. They were compared to 7100 babies who received MBM and formula. That group had a mortality which is similar to other published recent standards, a survival of 69% at 24 weeks for example, similar to the 70 to 80% survival for 24 weekers during the same years in the CNN.
The most likely cause of this increased death rate in the MBM + DHM group is Reverse Causation.
Dying will make you more likely to be in the MBM + DHM group, rather than the other way around.
Deaths in extremely immature babies usually occur early. Most babies do not receive fortifier in the first few days of life. Indeed many centres wait until an infant is on full feeds, or receiving 100 mL/kg/day, for example, before starting to fortify their milk. Death before receiving much feeds, if the baby is in a centre that provides DHM to very preterm babies, and does not immediately add fortifier, will place them in the MBM + DHM group.
Survival until on mixed feeds, with either fortifier, or the addition of formula, will therefore place a baby in one of the other groups.
I started to realize this by noting that the the major causes of late mortality were not much different between groups (NEC mortality 4% vs 0.5%, and late onset sepsis episodes, 8% vs 3%) even if all the septic babies died, there is still an enormous difference in mortality. Also, when I looked in the supplemental data there was another group of 1128 infants in the patient flow chart that were “nil by mouth over the entire stay” (NPO).
If the authors of this study did the same analysis of the babies who were NPO, I think we would find that their mortality was extremely high (maybe even higher than the MBM+DHM group!); not because being NPO caused them to die, but because dying put them in the NPO group.
Just as it is unlikely that receiving DHM was a cause of the increased mortality in the MBM + DHM group, but dying early put them in the MBM+DHM without fortifier group.
We have no idea of the survival of the other groups of different feeding approaches, but my guess is that they would mostly be similar to the MBM + formula group in the publication, as they will have survived long enough to receive fortifier.
There is another group of 484 infants referred to as “Did not receive any Own Mother’s Milk” which is differentiated from the other groups such as “exclusively formula fed”. Presumably the “did not receive MBM” group only ever received unfortified DHM. My guess is that babies whose mothers did not provide MBM, and who died before the milk could be fortified, would be more likely to be in this group. So this group probably had a very high mortality also.
The authors really need to redo this completely. They could present survival curves, which I bet would clearly show that the divergence in the mortality occurred very early. They could restrict the analysis to those babies who survived until they were off TPN, or were on full feeds, or whatever the database will allow.
Right now these data are unreliable, and risk creating major concerns about an intervention that the reliable data have shown to be safe and effective.
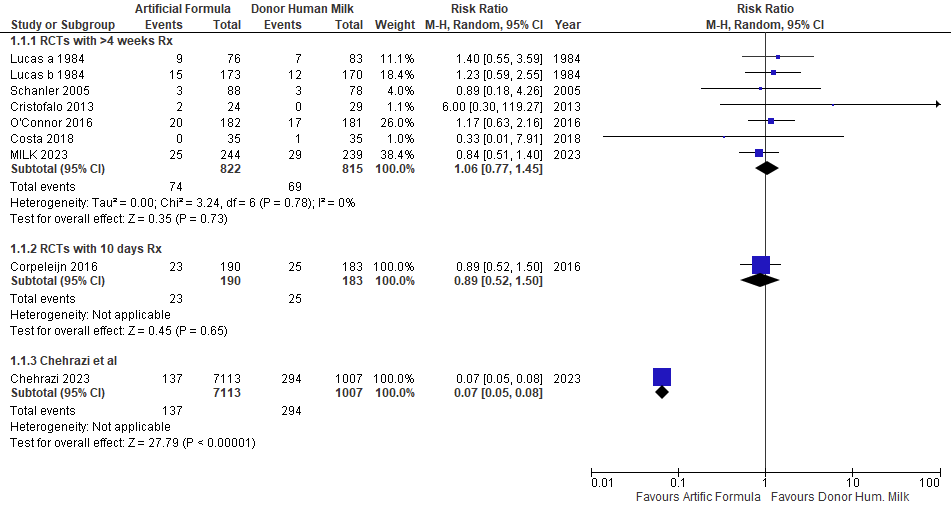
I have compared the results of this database analysis to the previous RCTs. With the addition of data from the MILK trial of the NICHD network, which has been presented, and the results are available on clinicaltrials.gov. That RCT in 483 infants <29 weeks who were not expected to receive MBM, compared formula to DHM, and showed no difference in mortality, but more NEC in the formula group, and no impact on long term developmental or neurological outcomes. I added their data to the studies in the Cochrane review, and put the Corpeleijn study in a separate group (as they gave DHM for only the first 10 days of life).
I know the authors of Chehrazi et al would never claim that it is equivalent to an RCT, but I just wanted to demonstrate how aberrant these data are.
Here is the comparison between the all-cause mortality in the RCTs and the new study
And here are the NEC results (of course Chehrazi et al reports only surgical NEC)
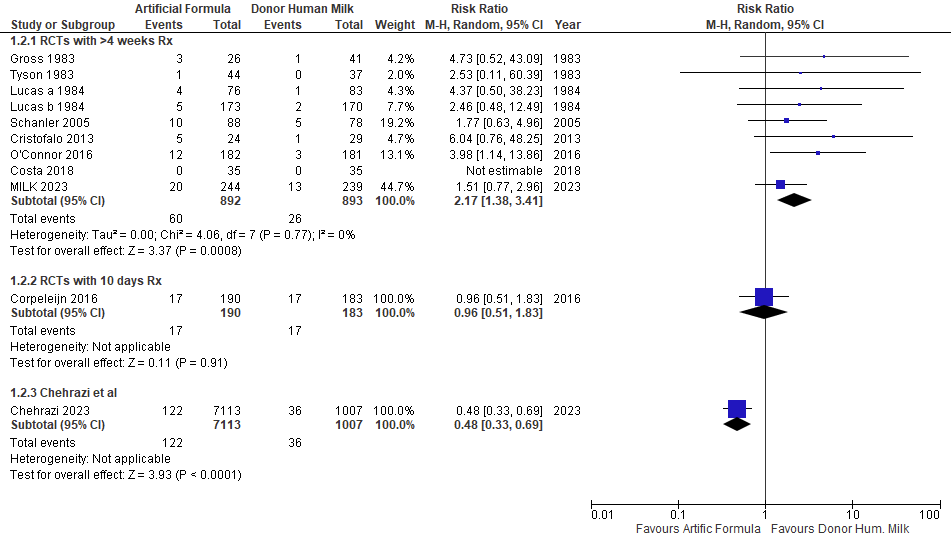
Both figures show that the Chehrazi data are profoundly different to the reliable data from the RCTs, which remain the only way to show causation, in the right direction!







Pingback: Donor human milk, not toxic after all! | Neonatal Research