
The recent statement from the AAP and a recent review article both state that probiotics only appear to be effective in babies over 1000g birthweight. This would be remarkable if it were true. I am trying to think of another intervention that is only effective in lower risk patients, and not in those at higher risk, and I am having difficulty. For most interventions, the relative risk is relatively stable across risk groups, that is one of the reasons for presenting RR rather than risk difference in meta-analyses, for example. The risk difference is highly likely to change according to the background risk.
In reality, most of the RCTs of probiotics have simply not reported their results divided by birth weight strata, but they have all included ELBW infants. Several trials have a mean birthweight of between 750 and 1000 grams, and thus more than half (probably) of their subjects below 1000g. Many others have mean birth weight between 1000 and 1200 grams, and have included many ELBWs. About 5/6 of NEC cases occur in babies <1000g (CNN 2021 report: 120 of 147 NEC cases in VLBW infants were in babies <1000g); it would be mathematically impossible for all the reductions in NEC due to probiotic prophylaxis to be among the >1000g infants!
This recent review article states the following, “Despite such evidence of significantly reduced NEC incidence following probiotic administration, most benefit accrues to infants with BW > 1,000 g”. They give 6 references to support this statement. Let’s actually look at that evidence. The first reference is to a network meta-analysis (Morgan RL, et al. Probiotics Reduce Mortality and Morbidity in Preterm, Low-Birth-Weight Infants: A Systematic Review and Network Meta-analysis of Randomized Trials. Gastroenterology. 2020;159(2):467-80) that does not mention subgroup analysis either by birthweight or gestational age. Not a good start. I checked the supplementary material also of that publication, and there is no such subgroup analysis.
The second meta-analysis referenced (Thomas JP, Raine T, Reddy S, Belteki G. Probiotics for the prevention of necrotising enterocolitis in very low-birth-weight infants: a meta-analysis and systematic review. Acta Paediatr. 2017;106(11):1729-41) found 5 RCTs that reported the efficacy of probiotics on NEC in the ELBW subgroup, 4 of which also reported subgroup all-cause mortality. Those 5 trials include a total of 1600 infants. If we actually look at these trials and their results, we find that all of them had similar outcomes in the <1000 and >1000 g subgroups. They all showed fewer cases of NEC with probiotics in the <1000g infants, although the differences were not “statistically significant”, the included studies either had very small sample sizes, or were the large UK study (weighted at 70% in the MA) in which there was only a very small effect of the B breve in the larger babies also. In other words, none of those studies give any credence to the idea that probiotics are more effective in larger babies, and less effective at <1000g. The other references given, in that recent review article, are to that same individual trial from the UK, and to the heavily criticised AAP statement, which relies on the same references.
In addition, the article references a cohort study from Perth, which showed a reduction in NEC among the <1000g babies from 19% to 5%! The relative risk was the same among the ELBW infants, and the VLBW infants as a whole; therefore the absolute risk reduction was greater in this subgroup, among the ELBW infants the NNT to prevent one case of NEC was 8.
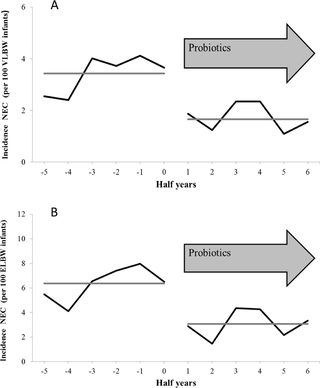
They also use, to support the statement that most benefit accrues to the larger infants, a reference to the large German Neonatal Network study (Denkel LA, et al. Protective Effect of Dual-Strain Probiotics in Preterm Infants: A Multi-Center Time Series Analysis. PLoS One. 2016;11(6):e0158136) which showed the same relative reduction in NEC among the ELBW and the VLBW (Hazard ratio in each subgroup was 0.48), and therefore a much greater absolute risk reduction among the ELBW. In that study the HR for mortality was 0.59 among ELBW infants with the use of probiotics (Infloran in the GNN units). The figure below shows the impacts in the VLBW (A) and ELBW (B) groups after the introduction of probiotics, which occurred at different points in the different participating NICUs.
Finally, that review article includes, as a reference to support the statement that probiotics are only effective above 1000g, the cohort study from the Canadian Neonatal Network, which only included babies under 29 weeks (Singh B, et al. Probiotics for preterm infants: A National Retrospective Cohort Study. J Perinatol. 2019). That study showed “The adjusted odds ratios of NEC (0.64, 95% CI 0.410, 0.996), mortality (aOR 0.41, 95% CI 0.26, 0.63), and a composite of NEC or mortality were significantly lower in the Probiotic Prophylaxis group”.
The most recent Systematic Review and Network Meta-Analysis that has been published, and which I have already discussed in the blog, (Wang Y, et al. Probiotics, Prebiotics, Lactoferrin, and Combination Products for Prevention of Mortality and Morbidity in Preterm Infants: A Systematic Review and Network Meta-Analysis. JAMA Pediatr. 2023) includes 80 RCTs with probiotics in one arm and placebo or no treatment in the other arm. I haven’t had time to look at why the difference in numbers of trials included, or the characteristics of the 13 trials that are in the NMA but not in the latest update of the Cochrane review. Wang et al showed a reduction of severe NEC with an RR of 0.38 for multistrain probiotics, and 0.13 for multistrain probiotics with HMOs. The risk differences were 3% and 5% respectively, summarized across all of the included studies in those 2 categories.
I find it very frustrating that the lack of subgroup data is interpreted, both by the AAP, and by other review articles, as meaning that probiotics may not work under 1 kg. The few RCTs that have reported such subgroups are either extremely small trials, or trials in which the effect in larger infants was very small, but in the same direction as the effect in the smaller babies. As I wrote at the start of this post, 5/6 of NEC cases occur in babies <1000g, it would be mathematically impossible for the reductions in NEC caused by probiotic prophylaxis to be confined to the larger babies, even if probiotics completely eliminated NEC in the larger babies.
Clearly there are enormous numbers of ELBW infants in RCTs that were just not reported separately. In the latest Cochrane review, 57 RCTs are included in the meta-analyses. But only 10 of them had data that could be included in the subgroup analysis of “ELBW or extremely preterm” babies (<28 wks), even though all of the trials included such babies. The total numbers randomized in the 57 trials included are over 10,000, but only 1800 were separately reported as subgroups in this category. The Cochrane review analysis of this subgroup, then, includes 6 further trials than the Thomas SR mentioned above, but excludes Lin’s trial (I can’t immediately see why Lin was excluded, as they did report outcomes by birthweight strata). The additional trials were all extremely small trials, with between 0 and 2 cases of NEC in each one, apart from Wejryd E, et al. (Probiotics promoted head growth in extremely low birthweight infants in a double-blind placebo-controlled trial. Acta Paediatr. 2019;108(1):62-9) which was a study of 134 ELBW infants randomized to receive L reuteri or placebo, in whom there were 7/68 cases of NEC in the probiotic group and 8/66 in the controls.
What about other therapies that we use, and which everyone employs regardless of whether the babies are over or under 1000g?
Lets consider delayed cord clamping in the very immature infant. The extensive NMA of Jasani et al examined the data available under 29 weeks which is presented in their supplemental information
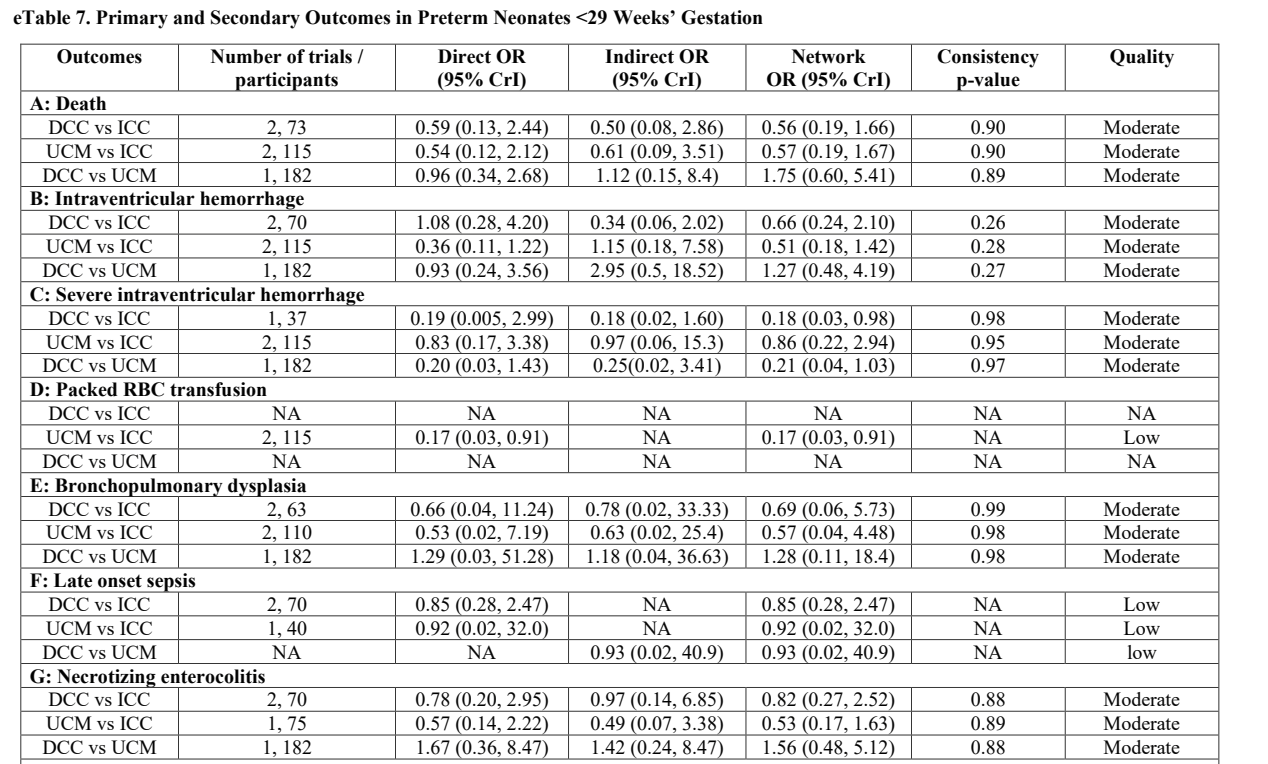
As you can see, there is no reliable evidence that DCC is safe or effective < 29 weeks GA. None of the outcomes are even close to statistical significance, with wide confidence intervals of the OR on either side of 1.0.
Should the AAP not follow the same reasoning as for probiotics, and note that DCC is of unproven value for infants <29 weeks?
I am obviously, (I hope it’s obvious), being sarcastic here to make a point. If we remember, the largest and best of the DCC trials in the preterm, the APTS trial, enrolled only infants <30 weeks gestation, but they did not report the <29 weeks group as a separate group. Therefore, when the authors of the NMA searched for data on known subgroups < 29 weeks they were unable to find more than a tiny amount of information. I don’t think there is any doubt that DCC has the same benefit among infants <29 weeks as it does if you put the cutoff at 30 weeks.
How about caffeine? The evidence supporting the efficacy of caffeine therapy for clinically important outcomes is largely based on the CAP trial of infants under 1250g birthweight. We did not report the effects on the subgroup of those of under 1000g. The Cochrane review has no data for babies under 1000g.
This is horrifying! We are using this medication, which is proven to work in babies <1250 g, to treat large numbers of babies <1000g but “current evidence does not support the use of caffeine for babies <1000g”, we could say, if we followed the same reasoning as for probiotics. The most immature babies are probably at greatest risk of the potential long term adverse effects of adenosine receptor blockade, should we not demand more placebo controlled trials of caffeine among the most immature babies? And stop using caffeine until we have the results?
Should the AAP also not follow that same reasoning for caffeine as they do for probiotics, and note that there is no reliable information about the efficacy and safety of caffeine in infants <1000g? FDA approval of caffeine is solely for infants >28 weeks. Many babies have died after receiving caffeine, some of whom were tachycardic, a known possible complication of caffeine. Indeed in the only, very small, trial of the approved version of caffeine in the USA, “Cafcit”, there were many more cases of NEC in the caffeine group. I am certain that there have been many infants who received Cafcit then developed NEC and died, should the FDA not follow the same reasoning, and warn everyone that use of caffeine <28 weeks is not approved and threaten the manufacturers with dire consequences if they continue marketing the drug for use in the extremely preterm?
Of course, we know that there were many <29 weeks babies in the trials of DCC, and there is no reason to believe it improves outcomes only among the bigger babies, despite the lack of data on the specifically <29 week subgroup. Many of the infants in the CAP trial were <1000g, and we have no reason to suppose that caffeine only works at >1000g.
In the same way, there have been thousands of babies <1000g in the RCTs of probiotics, and there is no good reason to suppose that they are only effective in larger babies. The absolute benefits of probiotics are likely greater among infants <29 weeks, or less than 1000g. That indeed is what the 2 cohort studies referred to above showed.
Overall, according to the pooled data from the latest NMA, for every 1000 babies who receive probiotics there will be about 30 fewer cases of NEC, 16 fewer deaths, and 25 fewer cases of late-onset sepsis, taking the data from the trials of multistrain probiotic mixtures.
The incidence of sepsis caused by the probiotic organisms is at present uncertain, there have been a few reports, which have been summarized, but the denominator for this total of 32 cases is uncertain. But, even if the incidence is high, at say 1% of those receiving probiotics, it remains the case that overall there are fewer deaths, and almost certainly less total late-onset sepsis. That incidence would mean that for every 3 cases of NEC prevented, and for every 2 deaths prevented, there is one case of probiotic bacteraemia, which is usually easily treated with beta-lactam antibiotics.
The risk-benefit of probiotics is clearly in favour of continuing routine administration in the very preterm, and there is no reason for excluding the extremely preterm from those benefits.
Please read this impassioned article by a mother who lost her son to complications of NEC, she went on to found the NEC society, dedicated to “Building a world without NEC”. A goal we can all adhere to, and one which has just moved further away because of the actions of the FDA.







Thank you for this — the “lack of data” for use of enteral probiotics to prevent NEC in <1000 grams has been a bit frustrating, and biologically confusing.
From a single center experience, the data published in Tobias et al (2022; DOI:https://doi.org/10.1016/j.jpeds.2021.12.070) showed a statistically significant reduction in NEC in ELBWs — on the order of 4 fold. Honestly, it was this effect that was the most notable. It is also the most worrisome group after the FDA warnings.
Of course, this is likely also the group with more risk for a probiotic strain finding its way past an intestinal epithelial barrier into the bloodstream — but again, as you have pointed out, as well as others, what is our risk benefit tolerance? I fall clearly on the same side as you.