
Many important trials include follow-up to about 2 years in order to ascertain longer-term effects. Such as this one:
Adams-Chapman I, et al. Neurodevelopmental outcome of preterm infants enrolled in myo-inositol randomized controlled trial. J Perinatol. 2021. Ira Adams-Chapman was one of our fellows when I was in San Diego; a wonderful gentle person, who would nevertheless stand up for herself, and for what she thought was right for her patients. I was never able to publish the study in piglets that we did together during her fellowship, as there were several technical issues that we couldn’t correct, but that didn’t stop her (or maybe even helped her!) becoming an important part of the neonatal world. After graduating from our program, she developed her research career in the follow-up arm of the NICHD network. I kept intermittent contact with her over the years, and remember a very pleasant breakfast in Atlanta when I visited a few years ago.
I was stunned to hear that she died towards the end of last year, far too young, having been predeceased by her husband, also far too young.
I mention this because I was pleased to see that, despite being unable to sign off on the manuscript which was submitted shortly after her untimely demise, she is still listed as the first author. I am sure that represents her contribution to this article, and to the high-quality work it represents.
The study is a report of the longer-term outcomes of infants enrolled in a trial of prophylaxis with myo-inositol for retinopathy prevention. Phelps DL, et al. Effects of myo-inositol on type 1 retinopathy of prematurity among preterm infants <28 weeks’ gestational age: A randomized clinical trial. JAMA. 2018;320(16):1649-58. At 2 years of age survivors were examined with the usual panoply of neonatal tests.
The new article notes that there was no difference in the composite outcome of “death or NDI” at 2 years corrected age mong survivors (95% of whom were evaluated; great work!) Which might suggest that either giving inositol or not were equally valid choices. But hang on, mortality was quite a bit higher in the inositol group, 20%, than the controls, 13%. The relative risk of dying was 1.53 (95% confidence intervals 1.08–2.18).
49% in each group of those followed up had neurological impairment or developmental delay (NIDD I will call it) and the summed outcome of NIDD or death was 60% (inositol) vs 56% among controls. As usual, infants with Bayley motor or cognitive scores <85 were the majority of those that had what they call “NDI”.
These results are a perfect example of why we should NOT be using “death or NDI” as the outcome for clinical trials.
More of the control babies survived, but the proportion of survivors with “NDI” was identical in the 2 groups, there were, therefore, numerically, more survivors with “NDI” in the control group, because there were more survivors!
When you then calculate the proportion of survivors without NIDD in the 2 groups, there is no “statistically significant” difference. Here is what that means for this study; in the Inositol group there were 62 deaths, and 14 babies not followed up, among the 289 babies with 2-year outcomes there were 112 with NIDD. In the control group, there were 39 deaths, and 14 babies not followed up, so among the 289 babies with 2-year follow up there were 122 infants with NIDD. This is my graphic of those results, the vertical axis being the absolute numbers of subjects.
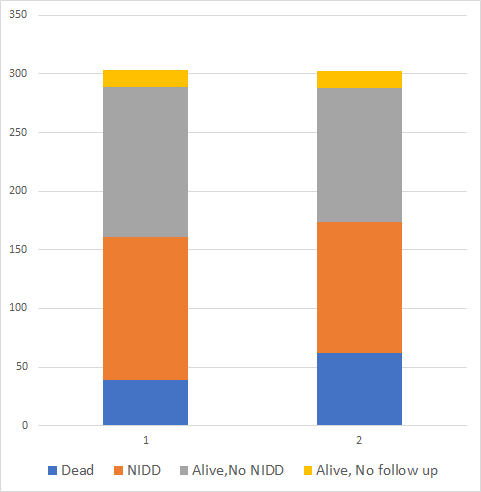
If you were to choose betwen treatment 1 and treatment 2, with substantially more deaths in group 2, and exactly the same proportion of infants with low Bayley scores among survivors, I bet there are not many who would choose treatment 2!
But the abstract of the article just notes: “Treatment group did not affect the risk for the composite outcome of death or survival with moderate/severe NDI (60% vs 56%, p = 0.40)” which suggests that the results are equivalent and that it doesn’t matter which treatment you choose, but which is entirely the wrong interpretation of these data.
For this particuar trial we do have the intial study report which noted that “death or RoP” was more frequent in the inositol group; but other trials may have “death or NDI” as the primary outcome, and many people would read no further than the abstract noting no difference in the outcomes.
From a strictly scientific point of view, one should not change the primary outcome after the data are in; so from that point of view, if the initial plan for the analysis was to compare “death or NDI” between groups, then that is what should be published, and the results as published are accurate. But, from the perspective of someone wanting to determine the best treatment choice for a baby, this is totally wrong; dying and having a low Bayley score are in no way equivalent. The analysis plan should take that into account, giving much more weight to survival than the results of screening tests for developmental delay.
Are there any outcomes that can be balanced against survival? The few studies that have asked this of parents note that they generally think that survival with impairments so profound that the child is unable to communicate would be a category equivalent to mortality. Such outcomes are so rare in the NICU that they will likely never balance differences in survival.
The same considerations apply to any screening test for developmental delay, not just the Bayley; but also to neurological impairment, even if likely to be permanen. Is cerebral palsy with a GMFCS of 3 equivalent to being dead? Is blindness equivalent to being dead? Surely, if they are not equivalent we should design our studies and our analyses to acknowledge that.
Children with impairments have lives that are worth living, and enrich the lives of those around them, despite the major challenges they also bring. I was reminded of this, and also of how bad we are in predicting whether a child will not be able to communicate, when I recently watched this video from ‘Britain’s got talent”
I love that song and that performance. Valuing children (and adults) for who they are regardless of their impairments is the moral of that wonderful anthem. If you only have time to watch the song, it starts at 2:20.







Thank you for this posting!
On Thu, Apr 22, 2021 at 12:24 PM Neonatal Research wrote:
> keithbarrington posted: ” Many important trials include follow-up to about > 2 years in order to ascertain longer-term effects. Such as this one: > Adams-Chapman I, et al. Neurodevelopmental outcome of preterm infants > enrolled in myo-inositol randomized controlled trial. J Perinat” >
Thank you for this very important discussion (and the wonderful video)!