
One recent publication states that 30% of all their babies under 30 weeks gestation had Acute Kidney Injury (AKI from now on). Another from a couple of years ago reports 40% of all their babies under 1500g had AKI.
Both of these publications based their definition of AKI on an increase in serum creatinine concentrations, an increase of over 0.3 mg/dl (that is about 26 micromol/L in modern units). Both of them included very preterm babies in the first couple of days of life. Both of them ignored the usual increase in creatinine that occurs during the first 2 to 3 days of the very immature infant.
The increase in serum creatinine has been described for several years, (Miall LS, et al. Plasma creatinine rises dramatically in the first 48 hours of life in preterm infants. Pediatrics. 1999;104(6):e76.) the mechanisms have been investigated (they include creatinine re-absorption from the tubules) and the usual profile of creatinine clearly described. This is what normal creatinine values in very preterm babies look like, according to (Thayyil S, et al. A gestation- and postnatal age-based reference chart for assessing renal function in extremely premature infants. J Perinatol. 2008;28(3):226-9).
.
. 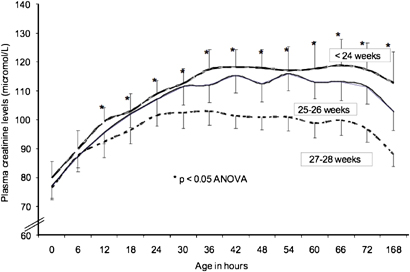
As you can see, on average plasma creatinine increases by about 40 micromol/L in the first 48 hours of life, which means, according to the definitions used in several recent articles, on average all very preterm babies have AKI!
The day to day changes were plotted like this (in the same publication).
So you can’t use a definition based on creatinine alone to diagnose AKI in very immature infants. According to one recent publication, 100% of babies at 22 and 23 weeks gestation had AKI, and 80% of 24 week infants. Most of those babies have good urine output, follow the usual postnatal weight loss trajectory, do not become hyperkalemic, in short they have no sign of renal dysfunction.
By day 2 to 3 tubular creatinine reabsorption is ending, and the creatinine starts to fall, after that you might be able to diagnose AKI from changes in the creatinine concentration alone, but it would be great to have some definition of AKI in the preterm that actually reflected renal injury and which was correlated with later renal problems, without that, it is hard to know what to do about a creatinine increase. Certainly creatinine increases in the first 2 days of life are almost universal under 28 weeks and do not mean Kidney Injury. Some years ago it was suggested that an increase in creatinine over 0.5 mg/dl, or 44 micromol/L could be used in the first 3 days, these graphs show that would be a more appropriate threshold, at least from a statistical point of view, if such a threshold is a good discriminator between those babies with and without true AKI needs to be investigated.







With much interest, the information you provide and your perspective is much appreciated. A few comments. We don’t truly understand the reasons why serum creatinine rises in such a way in the most extreme premature infants. Besides the possible reasons listed above, there is probably a “finding a new normal” that reflect the babies homeostasis after birth. In addition, the impact that rapid shifts in fluid has on serum creatinine (independent of kidney function ) may be substantial. We have recently published on this in pediatric nephrology 2016 (in press). However, those interested in improving our understanding of how to best define neonatal AKI, bust understand a few things…
1. we have to have an empiric agreed upon definition, otherwise, we will have the ability to compare studies where one uses definition 1, and another investigator uses definition 2. At the NIH sponsored Neonatal AKI symposium, the definition used in these studies was felt by a panel of expert to be as good or better than any others that have been proposed.
2. This empiric definition has NOT been tested to predict clinical outcomes, nor has any other definition. In order to make progress and find the most valuable method for diagnosis of neonatal AKI, neonatologist and nephrologist MUST work together to perform large, adequately sampled studies to determine if this (or other) definitions best predict clinical outcomes, and perhaps more importantly, can provide us with a timeframe where a tested intervention can have an impact on the short and long term outcomes of these vulnerable infants.
3. The AWAKEN study performed by the Neonatal Kidney Collaborative (NKC) , has not collected data on over 2100 neonates who met inclusion and exclusion criteria specified. Over 350 variables have been collected for each infants. The Repaired study is an ancillary study being conducted on 1000 infants randomized in the PENUT trial. We anticipate that these cohorts will help us improve the understanding of how to best define Neonatal AKI. .
Your comments are well noted, but they are also based on a lot of assumptions and some potentially inaccurate theory dating from the late 90s.
You discuss about how “creatinine reabsorption occurs from the tubules”– Just so you know, there is no transporter nor mechanism for creatinine to be reabsorbed, ever… so that’s a pretty unusual mechanism to claim without direct evidence supporting it.
I don’t mean to be cynical, but rather I think we should reconsider this important question. You describe a graph that shows creatinine levels rise in preterm neonates. This was from data from 1999. On one hand, this could be a physiologic response in the premature neonate. On the other hand, if 30-40% of neonates were to actually have AKI, then wouldn’t a population of pre-term neonates have a rising creatinine? Someone needs to study that to distinguish the difference (knowing what we know now; and what we didn’t know in 1999). How do we know that the plot, which was felt to be normal response in 1999 is actually normal? (especially if the proposed basis was a creatinine “reabsorption”?)
You describe “the mechanisms were proven” — well I followed that link and they describe an animal study in rabbits– infant rabbits vs adult rabbits comparing Creatinine clearance to Inulin clearance. There is a difference and creatinine clearance is lower– so the authors of that study claimed this was “explained by reabsorption of creatinine at the renal tubule.” Yet they make this claim without any study of the renal tubular functions. There are no renal tubular experiments to demonstrate that this was in fact due to “creatinine reabsorption”– they seemed to just come up with that explanation on their own, to explain the decreased creatinine clearance compared to inulin clearance.
So there’s something there, and I could think that there may be less creatinine secretion in the premature renal tubular and that could explain things sufficiently, making this rise a “physiologic” one (rather than from AKI). However, rather than calling it normal, perhaps someone can actually study this? We are seeing AKI in premature neonates leading to significant long-term effects when they are teens and young adults. Neonatologists are saving lives and that is amazing but now that they are being saved we can truly investigate means to save them and make them healthier and happier into adulthood as well!
I agree, clearer and more evidence based definitions of AKI in the premature neonate are sorely needed.
Great points…completely agree!
Taking into account the acute changes in weight may help us understand what is happening to the creatinine in the first few days…Ultimately, urine biomarkers will likely help us determine if damage has occurred….http://www.ncbi.nlm.nih.gov/pubmed/26572893
Two quick comments:
1) “This is what normal creatinine values in very preterm babies look like.”
I disagree. Extremely premature neonates are in a decidedly abnormal physiologic environment – so defining a “normal” range for creatinine is challenging, to say the least. Yes, we can draw a 95% confidence interval around the typical creatinine values we see in the NICU. But there’s an important distinction to be made between “normal,” meaning commonly observed, and “normal” meaning indicative of good health. For instance, it’s “normal” for a 24 weeker to be intubated – but no one would claim those babies aren’t at risk for both short- and long-term morbidity and mortality.
2) “It would be great to have some definition of AKI in the preterm [neonate] that actually reflected renal injury and which was correlated with later renal problems.”
I couldn’t agree more with the first part. Even when normal values are clear, serum creatinine is a marker of renal function – not injury. We still need the “renal troponin.” Until then, we can only diagnose AKI when an injury is so severe that the kidney’s function becomes impaired.
I disagree (at least somewhat) with the second part of the statement. It is true that no definition for AKI is well validated in neonates. Whether a 0.3 mg/dl rise in serum creatinine is meaningful for preterm neonates is admittedly unclear. But it is absolutely true that any neonate who develops stage 3 AKI at some point prior had stage 1 AKI. Recognizing AKI earlier may give neonatologists the opportunity to intervene sooner and improve care for these babies.
Great points dr Carmody –
One could argue that every premie has abnormal function and inappropriate ability to maintain homeostasis.
Another comment about the incidence of neonatal aki….most of the studies in neonates to date rely on clinically based measures of kidney function – so the estimates provide conservative number whereby there is an assumption that those who don’t have labs check did not get aki – just cause one does not look for a problem does not mean that a problem is not present ….
This is a great discussion; a few points I’d like to make, the data in the graphs are not from 1999, but from a publication in 2008, based on data from between 2001 and 2004. I don’t think the care of very immature infants has changed much since then, mortality certainly hasn’t changed much. The babies were nursed in humidified incubators, with other details of their fluid balance being rather standard.
It is of course true that all babies born at 24 weeks are “abnormal” there is no true “physiology”, rather it is all patho-physiology. Nevertheless most very immature babies do not develop severe AKI, so how frequent is milder AKI, and how do we diagnose it? We know that GFR is very low in the fetus, and increases rapidly after birth at term, and in experimental mammals; the usual profile of GFR changes after birth has not been studied much in very immature babies, indeed I don’t know how that we be done, unless you could find a non-invasive way of doing it,
The statement about creatinine “reabsorption’ is as you all know based on the work of authors who showed that creatinine clearance in neonatal mammals was lower than Inulin clearance. The only explanation that I have seen for that is that there is some passage of creatinine out of the tubules; perhaps a tubular leak, rather than reabsorption is better terminology, as I recognize there are no receptors for creatinine. As I mentioned I don’t see how it helps to diagnose 80% of 24 week infants as having AKI, if there are no clinical consequences of the increase in serum creatinine, if the creatinine almost always increases in these babies, and then spontaneously falls again without specific intervention, and there is no clear link between increased creatinine and longer term renal issues, then to consider it “patho-physiologic” and part of the usual adaptation to extra-uterine life of the very abnormal profoundly preterm baby, is to my mind more helpful than labelling it as AKI using criteria which were not developed for such infants.
Pingback: Interesting comments | Neonatal Research
Pingback: Renal Function in the very immature preterm, what is a “normal” creatinine | Neonatal Research