I was disappointed to not be able to go to PAS this year, mostly because I am privileged to have a circle of former trainees, colleagues and friends from around the world who are all involved in trying to improve care for newborn infants. I love meeting up with you all every year, and after the pause caused by COVID it would have been great to see so many of you. Still someone has to look after the babies. I decided to give myself a reward and go on a birdwatching trip on Monday, travelling to Baie du Febvre, on the St Laurence about half way between Montreal and Quebec. It is one of the staging spots for the Snow Geese on their return from the south as they head to colder climes. In addition to about 10,000 Snow Geese I was pleased to run across this fella
He seemed to want to pose for his portrait, so I got my first ever shots of a Snowy Owl. Then he decided to fly off just as my memory card was getting full.
In addition there were a few purple martins, who come back earlier every year with climate change, and many tree swallows, like this one, who are building nests as they prepare for egg-laying
Other recent firsts for me were a Barred Owl at the Montreal Botanical Gardens
And Sandhill Cranes singing to each other (not very musically)
They stand about 1.5 m tall when they stretch their heads up like that, towards the other end of the scale is this Brown Creeper, about 12 cm from tip of beak to end of tail
Maybe next year after PAS I can post some selfies with my buddies!
The scientific basis of neonatology is vitally important to me, the enormous advances that we have made have all been founded on basic and clinical science. So I can get quite agitated when I see articles reporting trials of interventions for which there is no rational scientific basis, especially when they are published in reputable journals. This study for example in the Archives of Disease in Childhood, investigated whether osteopathic manipulation would improve the frequency of exclusive breast feeding. (It didn’t) If you don’t know much about osteopathy, maybe that would sound reasonable, but osteopathic manipulation is a practice with no scientific basis.
Osteopathy was invented in the 1870s by a charlatan called Andrew Still, who pretended to have medical training, and came up with vague beliefs that all human illness could be treated by manipulation adjusting the nerves and muscles. He reported his own forays into treating children, including a comment in his biography that he could “shake a child and stop scarlet fever, croup, diphtheria, and cure whooping cough in three days by a wring of its neck”. The scientific underpinnings of osteopathy have not advanced since then.
One could ask, for a study such as the one I opened the post with, if performing a negative study is a good thing, as it might convince people not to have their babies manipulated. Perhaps well-performed studies in countries where a lot of people already use osteopathic practitioners might be a good way to guide people away from them. I think that is extremely unlikely to be effective, despite the complete lack of a scientific basis for the practice, many people consult osteopaths, and I think recent experience has shown that regardless of how ridiculous the quackery you can find people defending it with very loud, effective pulpits on social media. I think, in contrast, performing such studies gives a veneer of scientific credibility that is unjustified, it is better to say from the start, that osteopathy is a practice based on the pre-scientific notions of a 19th century charlatan, and it should not be given any credibility.
If you want to see how ridiculous this continues to be, watch a few youtube videos from proponents of osteopathy. Apparently osteopaths are able, by touching a baby, to determine if there are abnormalities of CSF circulation, (there always are) and fix the circulation by laying their hands in various positions and by pressure or traction create permanent readjustments. They seem to be heavily into craniosacral pulsations, which apparently have a frequency of between 6 and 14 per minute, and are imaginary, of course, but any osteopath able to pay their consulting room rent will reliably find abnormalities of the craniosacral mechanism and fix them with manipulation.
It was very easy to find promotional videos which show how an osteopath would manipulate a baby’s skull to adjust the parietals and occipitals (they tend to know a lot of anatomy words) to cure colic, one of them used a pleasant circular rocking technique, which looks like it would make the baby temporarily calmer, but create permanent physiologic changes, I doubt it.
A quick word about D.O. training in the USA, which is quite different to what osteopaths learn in the rest of the world. In general in the USA D.O. trained physicians go to accredited schools, with the same accreditation as for M.D. training, and they have licences and scope of practice identical to MDs. Their training is just about identical also, with maybe some extra emphasis on the muskuloskeletal system, but that is not what we see in Europe, or Canada, where osteopathy practitioners have no relevant medical training.
Unfortunately the Journal of Osteopathic Medicine has its own youtube channel, with instructive videos about, for example, how the Galbreath technique of skull manipulation is supposed to permanently adjust the drainage of the Eustachian tubes and treat otitis media. Otitis media is over-diagnosed and over-treated with antibiotics, probably, anyway, so perhaps a bit of placebo manipulation might not be a bad thing! (That is a light-hearted comment, evidence-based otitis media evaluation and treatment is important). But when we come to infants, being treated for real problems where effective therapies exist, using ineffective manipulations or treating imaginary problems will not improve their health.
This amazing example (Osteopathic manipulation improves cerebro-spanchnic oxygenation in late preterm infants) was published in the journal “Molecules” which is a journal from MDPI, previously listed as publishers of predatory journals in Beales’ list: in this study the authors placed cerebral and splanchnic NIRS sensors on 7 day old late preterm infants, then performed manipulations while watching the NIRS signal. Regional splanchnic saturation decreased and calculated oxygen extraction increased while they messed about with the babies. They interpreted this as a good thing! Will you tell them or shall I? I think they should ask for a refund of the 2,300 Swiss francs they seem to have paid to get it published.
But it can get worrying, a prospective trial of osteopathic manipulation in asphyxiated babies post cooling was performed, in a hospital in the USA, one of the authors is from the hospitals “manipulation service”. Each of the 12 carefully selected enrolled babies was compared to 3 historical controls; even with this piss-poor study design they were unable to show any effect on length of stay, which was their outcome. But, low and behold, they did show that “by the final treatment, the craniosacral mechanism’s intraosseous and cranial base compressions and physiologic motion were improved”, so that’s good.
The authors also claimed that although there was no statistically significant difference in length of stay (9.1 days vs 10.1 days) it might be “clinically significant”. Fortunately this drivel was published in a journal called ‘the Journal of Osteopathic Medicine” so probably no-one will take any notice of it. How is it possible, that these authors, 2 of whom seem to have appointments at Tuft’s, can really believe that by touching a baby they can determine the intraosseus craniosacral mechanism, and its physiologic motion? It must take a special kind of self deception to swallow this stuff.
A “scoping review” of osteopathy (Osteopathic Manipulative Medicine, OMM) in paediatrics was published in the journal “Pediatrics” last year. They were unable to find any reliable evidence that OMM is of any value. The review concluded that:
“There is little strong, scientific, evidence-based literature demonstrating the therapeutic benefit of OMM for pediatric care. No strong clinical recommendations can be made, but it can be medically tolerated given its low risk profile. High-quality, scientifically rigorous OMM research is required to evaluate safety, feasibility, and efficacy in pediatrics.”
No, no, no. The first sentence is a bit weak, but truthful. The second sentence should be “There is no rational scientific basis for any of the claims of OMM”, and the third “It would be a waste of resources and an abrogation of our duty of care to families to perform more research of OMM”. If future research can find a hint of a scientific justification for osteopathy, then prospective randomized trials could, theoretically, be designed which should be carefully masked and use sham manipulations in controls. But the science should come first, which is currently lacking, craniosacral pulsations anyone?
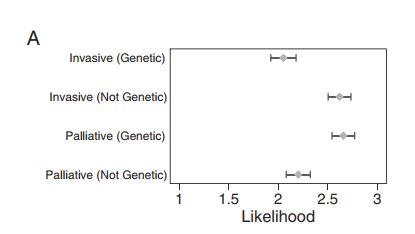
Just after I pressed “post” for a recent addition to the blog, I saw this appear. (Callahan KP, et al. Influence of Genetic Information on Neonatologists’ Decisions: A Psychological Experiment. Pediatrics. 2022;149). It illustrates some major problems in how neonatologists react to genetic information. The authors questioned a national sample of neonatologists about how they would react to some genetic information. The respondents were randomized and each received 4 clinical vignettes, either with or without some genetic information, the cases were designed to illustrate real dilemmas that we face in clinical practice. One case that was really concerning was concerning an extremely preterm infant with an unusually protracted resolution of his lung disease in whom whole exome sequencing had been performed, in one version of the case there was no diagnostic abnormality, in the other the sequencing revealed homozygous abnormality of uncertain significance in a surfactant protein gene.
I would have thought that a finding of “uncertain significance” should have no impact on treatment approaches or goals, but that is not what was found.
For this scenario, that figure shows that neonatologists who got the information that there was a variant of uncertain significance (“Genetic”) were more likely to desire palliative care, and less likely to recommend invasive interventions than those who were told the WGS was normal (“Not Genetic”).
My interpretation of the finding is that many neonatologists do not understand what a variant of “uncertain significance” means, and that we are in need of education.
The American College of Medical Genetics classifies genetic variants into 5 groups: pathogenic; likely pathogenic; of uncertain significance; likely benign or benign. The terminology “variant of uncertain significance” is used for situations where the variant is either previously unreported or there are not enough cases to know what the impact might be. Sometimes the genetic geniuses can guess that, for example, a mutation which leads to an early stop codon, in an essential gene with other known diseases associated, is likely to be pathogenic, even if it has never been seen before. But a variant of unknown significance could easily be a mutation with no clinical impact at all. Surely a variant of uncertain significance should have no impact on decision-making.
The discussion of this case is very illuminating : “For this case, respondents cited pain and suffering as more important considerations if they saw the genetic version of the case and were thus more likely to recommend palliative care. There is no reason to believe that a VUS would be associated with increased pain and suffering. This pattern is in line with previous work documenting that physicians cite quality of life more often when recommending palliative, rather than invasive, interventions. It is also consistent with reported use of suffering to represent the general utility of an intervention and justify a wide variety of decisions.”
That is certainly also my experience, when neonatologists think that we should continue intensive care we talk about chances of survival and long term outcomes, when we want to limit care we start talking about suffering. I don’t understand though why a VUS (variant of unknown significance) would have any impact on those considerations.
In another of the cases there was an incidental finding of William’s syndrome in an extreme preterm baby at 2 weeks of age with septic shock and severe respiratory failure, the “control” non-genetic version stated that the genetics test was normal. The baby needed a central catheter inserted for antibiotics. I would hope that, if that happened in real life, the neonatologist, if unaware of the real implications of William’s syndrome, would consult colleagues and discover that William’s syndrome is a condition with variable and relatively mild intellectual impairments and a range of other moderately serious medical problems. I would not have thought that many people would consider William’s syndrome an indication for limitation of care, but the responses to this case were similar to the first, and the graphic is almost identical, substantially more neonatologists would recommend palliative care if the genetic abnormality was diagnosed, than those who had the case scenario with a normal genetic test, and fewer would recommend having a central line inserted for the antibiotics. I find it disturbing, that a diagnosis of Williams syndrome, even in an extremely sick baby, would lead to a recommendation to not even insert a central catheter for antibiotics.
Genetics is a discipline that has advanced enormously since I was trained, and the advances seem currently to be exponential. It is not surprising that there is limited knowledge among neonatologists of what the implications of certain findings might be. It is incumbent on us to seek out those who really are knowledgeable if we get back a genetic test result that we are uncertain about, and certainly not make life or death decisions that are not rational, and are based on misunderstandings.
To return to a concern expressed in a recent blog, there are animal models and some observational data that suggest that antenatal steroids (ANS) could have a negative effect on cerebral development, at least with the doses used currently. Among very preterm infants this is probably overshadowed by the positive effects on survival, early neonatal adaptation, and reduction in intraventricular haemorrhage. But when the benefits are more modest and short term, one might ask if the risk/benefit is positive.
Almost all of the data are from observational cohort studies, and almost all of the data for infants born at term are from a single study, which I have mentioned previously, Raikkonen et al. Which means that the conclusions of the SR and meta-analysis are identical to the conclusions of Raikkonen.
At the very least, this analysis shows we must get better data. With so many babies exposed to ANS who later deliver at or near to term, if there truly is an adverse effect it is essential that it be accurately quantified. The modest benefit of ANS for late preterm deliveries, with an absolute reduction of 3% of babies with respiratory distress, coupled with the worrying data in this systematic review, also make it clear we should improve our efforts to focus ANS use in women who actually will deliver very preterm. For babies who do eventually deliver very preterm, the advantages, both in the short term, and as shown in this publication, in the long term, are clear.
Annie Janvier, John Lantos and I have just published an article about Next Generation Sequencing (Janvier A, et al. Next generation sequencing in neonatology: what does it mean for the next generation? Hum Genet. 2022), which is a common way of referring to rapid whole genome or whole exome sequencing. We hang the discussion on 3 cases from the NICU at my hospital, which all had certain similarities, they were term newborn infants with unexplained refractory seizures. In each case rapid next generation sequencing (NGS) was organised, and took 5 to 7 days to have a result. We did not have access to ultra-rapid sequencing, which, in some publications, can have a turn around time of about 72 hours. In all 3 of our case histories the NGS gave a result of compound heterozygosity of probably pathogenic abnormalities affecting a likely responsible gene.
Our discussion is focused on the following considerations: 1. A small minority of NICU patients have uncertain diagnoses; 2. among babies with uncertain diagnoses, a minority have a diagnostic finding on NGS; 3. among babies with a diagnostic finding, a minority have an impact of NGS on their therapy; 4. among babies with an impact of NGS, a minority have a therapeutic intervention that will improve their condition. Which might all sound like we are Luddites fighting against the inevitable, but each statement is based on evidence from the literature.
Most babies are in the NICU because of prematurity, sepsis, asphyxia or major congenital anomalies. Only the last of those are sometimes monogenic, as well as some of the remaining infants with, for example, unexplained hypotonia or seizures or multiple minor anomalies. In large published cohorts it is often not clear what the denominator was, in one study from the Netherlands, NGS was considered appropriate in 2% of babies admitted to the NICU.
The proportion of babies with a positive, possibly diagnostic, finding on NGS, among those considered for testing, is between 19% and 51%. It will obviously depend on the threshold for testing, if testing is applied more widely the proportion with a possibly diagnostic finding will fall. But the proportion with incidental findings will be stable.
In how many babies does a diagnostic finding have a useful impact on their clinical management? This question was the hardest to answer from our literature review, as the reported impacts on management, and how they were defined were often unclear. Very often, the purported benefits were very questionable such as “referral to an endocrinologist” or “prescription of salbutamol”. Some of the rationales smacked of genetic determinism, for example a case where a supraglottoplasty was avoided because the precise variant associated with the infant’s CHARGE syndrome was discovered. I don’t know about you, but I wouldn’t have a supraglottoplasty performed, or not, based on the genetic rearrangement, but on whether that individual child had airway obstruction likely to be improved by surgery. Two infants with identical genetic abnormalities may have very different phenotypes, which has been shown many times, even in cases of mono-zygotic twins with CHARGE.
Among those with a medically actionable genetic abnormality, it is an even smaller proportion who have a condition for which specifically tailored or curative treatment exists for the condition diagnosed. We found, for example, cases in the reported cohorts of Dravet syndrome and of hyperoxaluria where therapy was changed after NGS, but even those specific examples are cases where other children have been effectively managed without NGS. Which isn’t to say that there were no benefits of NGS, just that a more rapid diagnosis and tailored therapy should be balanced against the cost implications, and also any potential adverse impacts.
One of the most commonly reported “benefits” of NGS in the NICU is a recognition that a condition is uniformly lethal or refractory to treatment, leading to a redirection of the goals of care, with the suggestion that this can occur more rapidly when there is an NGS result. In contrast, we think that caregivers and families may become unwilling to withdraw life-sustaining interventions without the NGS results, which may well lead to delays in redirection of care, and periods of unnecessary NICU treatment. Unless you have the enormous funding required to perform ultra-rapid NGS on demand, then a delay of at least 5 days is likely; even with ultra-rapid NGS this will likely be 72 hours minimum. As the majority of NGS results do not produce an aetiologic diagnosis, it could well be that the most frequent result of performing NGS is a delay in the withdrawal of life-sustaining interventions.
Very often, in the published case histories that we tried to analyse, it did indeed seem that performing NGS just delayed withdrawal of such interventions when it was clear that it was already something that should be considered. Obviously the brief details in a publication covering multiple cases cannot convey the complexity of the interactions of the medical team and the family, but our own experience, as described in our cases, illustrates that as something that can occur. One of our cases developed an iso-electric EEG during the interval between sending the NGS and receiving the result. We could have, and some families would have requested, waiting until the result was available, our evaluation of the situation was that there were no diagnostic possibilities that could lead to a good outcome and the medical team and parents agreed to redirection of care without the NGS result. In our estimation, that case was actually one where the NGS was helpful, just not in a way that would have been considered in any of the published cohorts. The parents were very relieved that the diagnosis was found, which reduced their feelings of guilt, and allowed them to adapt.
Another of our cases had a very different result, with an NGS finding of a condition that would likely lead to profound intellectual limitations and behavioural problems, for that case the parents stated that knowing the results had seriously adversely impacted their ability to adapt as new parents. The third case had a sort of neutral result, the parents were content to have a diagnosis but it made no difference to them regarding how they wanted their infant treated.
All of the cases in our article had a result from the NGS that was considered to be “probably pathological” affecting genes known to be probably implicated. We selected those cases to make important points for our discussion, but they represent a small minority of NGS results. Much more commonly NGS does not provide a diagnosis. Also very commonly NGS results reveal possibly pathogenic abnormalities, or abnormalities “of uncertain significance”, which may make decision-making more difficult rather than more straightforward. In addition, there are, of course, the incidental findings of abnormalities in other genes that may have clinical significance for unsuspected conditions. About 5% of NGS in children, for example, reveals cancer susceptibility genes, which may be of benefit for the future of the child, but very often the benefit is currently unclear, and balancing adverse impacts have not been considered.
I was surprised recently to see a debate in the BMJ, with pro and con articles regarding the idea of universal whole genome sequencing as a possible new standard for neonatal screening. Even though the pro position did introduce some nuances, and suggested a progressive revealing of results of Whole Genome Sequencing according to which results an independent panel would consider relevant at different ages, it still seemed to me to be motivated by the kind of genetic determinism that I mentioned above. The authors seem to believe that a genetic abnormality equates to the diagnosis of a disease state, and that revealing a diagnosis will improve health outcomes. Let me give you one counter example, discussed by John Lantos in his article The False-negative Phenotype. This is an example for just one genetic anomaly, Krabbe’s disease, in which universal screening in New York state commences with a screen for the metabolic abnormality (low galactocerebrosidase levels), and, among those who are proven to have the biochemical abnormality, then sequences the gene responsible. Ninety percent of babies who are identified as having both the biochemical abnormality and the genetic defect remain asymptomatic. This disease was previously thought to be just about universally lethal, but with screening we now know that is not true. It is also unclear how many babies without the biochemical abnormality have the gene defect; so what should we do when a baby is identified as having the genetic abnormality that causes Krabbe’s disease? There are many other examples (perhaps none so striking) of genetic abnormalities which are thought to be clearly pathogenic being discovered in individuals who do not have the disease thought to be caused by that abnormality, some other examples are discussed by Dr Lantos in that article.
The pro article in the BMJ does not mention that as a concern. They also state that “extensive clinical evidence has shown that screening for genetic diseases saves lives. Research has shown that it can be cost effective”. Those 2 assertions should be challenged, In answer to the first assertion, yes, screening for phenylketonuria saves lives and brain cells, screening for cystic fibrosis improves pulmonary outcomes, many other examples are available, but neither of those examples rely on genetic screening, they actually rely on detecting the presence of the disease, which, I reiterate, is not the same as finding the presence of the genetic anomalies. In support of the second assertion they reference an article which does not support their assertion! The referenced article in question models the cost-effectiveness of informing patients about a series of 56 incidental findings which the College of Medical Genetics in the USA recommend informing patients about if they have genomic testing. What the study actually found was that informing asymptomatic adults about those 56 findings was NOT cost-effective (unless the NGS was very cheap). With universal NGS of asymptomatic babies, of course, every finding will be an “incidental finding”, which will lead to an enormous increase in workload for our genetic counsellors and clinical geneticists. The additional complexity which is added by the fact that huge numbers of genetic variants are of “uncertain pathogenicity” or may be reclassified from being “likely pathogenic” to “likely benign” as more data accumulate, makes the idea of universal sequencing of the whole genome a non-starter.
My recent experience of highly selective NGS has sometimes revealed important diagnoses, and had a benefit for families with a diagnosis. In one case, for example, of an infant with multiple apparently unrelated disorders the diagnosis of MIRAGE syndrome (that I had never heard of) was helpful to stop us searching for other causes. Supportive treatment of each of the problems was organised, and the family were relieved to have an answer. There was, as usual, no specific treatment, but as mentioned that is an extremely rare result of NGS. On the other hand, some families are relieved to hear that the NGS is negative, and that their baby’s problems do not appear to have a genetic cause, that is also a potential benefit.
The message of our article is that the potential and real benefits to some families should not be exaggerated. An appraisal of the value of selective NGS, or of the idea of universal NGS, requires a realistic evaluation of the benefits and also of the adverse impacts on some families. I don’t think NGS will ever be cost effective if you calculate the benefits as QALYs gained, there are so few babies for whom a genetic diagnosis leads to a life prolonging treatment, or a life improving treatment. The very real benefits for some families are much less tangible and impossible to cost. But we must not forget the potential harms also, in order to find ways to minimize them. The advent of truly effective gene therapies (most recently for sickle cell disease) suggests that in the future there may well be a substantial group of conditions which could be treated in presymptomatic babies; that may become another argument for universal NGS screening. Until that happens, and until we figure out how to pay for all the gene therapies that are on their way, I think we should stick to highly selective NGS, and recognize the enormous difficulties in the informed consent process.
In response to my previous post about preterms smoking I was directed to a recent publication about the issue, Notley C, et al. Development of a Smoke-Free Home Intervention for Families of Babies Admitted to Neonatal Intensive Care. Int J Environ Res Public Health. 2022;19(6). Although the title of this post refers to preterm babies, because I linked my previous concerns to the potential deterioration of lung health in former preterm born adults, the publication deals with all babies in the NICU. As the authors of this study note, maternal smoking during pregnancy increases the chances that their infants will be admitted to the NICU. And even though smoking has become much less frequent over the last couple of decades, there are still between 10 and 18% of adults who smoke in Quebec depending on age group (2020 data from Stats Canada). Probably, therefore, around 20% or more of NICU parents smoke here, and improving the respiratory health of all our NICU graduates will be very dependent on protecting them from environmental smoke.
The smoke-free intervention that was evaluated was as evidence-based as possible, following a systematic review (Brown TJ, et al. Systematic Review of Behaviour Change Techniques within Interventions to Reduce Environmental Tobacco Smoke Exposure for Children. 2020;17(21):7731). Most stopping smoking interventions are disappointing in terms of efficacy, so any intervention should be as evidence-based as possible, to select those features for an intervention which might work. Nicotine is incredibly addictive, with most smokers having great difficulties in quitting. Brief advice, group support or individual “buddy” support, nicotine replacement therapy and a couple of medications have been shown to have some effect. Increasing cigarette prices is one of the most effective, but not something we can have much impact on! Interestingly, it seems that brief advice (less than 30 seconds) is at almost as effective as longer lectures… Probably a more widespread lesson there.
At a minimum, we should ensure that all parents taking home a baby from the NICU have been questioned about their smoking status, have brief advice to inform them that it is a risk factor for themselves and for their baby, and are given access to smoking cessation resources. In the paper which I reference at the beginning of this post, they held interviews and focus groups with parents and health professionals; “Findings demonstrated that both parents and healthcare professionals supported the need for intervention. They felt it should be positioned around the promotion of smoke-free homes, but to achieve that end goal might incorporate direct cessation support during the NICU stay, support to stay smoke free (relapse prevention), and support and guidance for discussing smoking with family and household visitors.” In general, parents will likely be open to being questioned about smoking, and will appreciate a more global approach to the health of their family after discharge.
To many followers of this blog, the title may seem a little strange; is there any difference? Surely science underlies all of our field, and testing treatments in adequately designed trials leads to progressive improvements through the application of evidence-based therapies.
In general, the evidence-based therapies that we have in our field have been based on scientific understanding, basic biochemistry, developmental biology, and so forth, which has led to the development of therapies (I am thinking of surfactant replacement as the shining example) which have then been proven effective in clinical trials. This particular therapy was developed from observations of the role of surfactant in the lung, evidence that infants with HMD lack surfactant, investigations of the various components and development of stable mixtures, which were then tested in animal models, and finally in large multicentre RCTs and showed efficacy. The vital importance of EBM is shown by some counter examples; as one example, the use of immunoglobulins as a treatment of neonatal sepsis had a reasonable scientific basis, with preterm babies have very low Ig concentrations, and knowing that immunoglobulin deficient older children were at very high risk from sepsis. However, the pivotal trial of IgG supplementation was negative.
The problem with evidence-based neonatology, without a science-based foundation, is that interventions without any prior plausibility can be tested, just because someone thinks that maybe it could be a good idea, but without a reasonable scientific basis. Because there has not been an RCT it could be considered that there is no evidence to decide whether an intervention is effective or not. This can lead to the ridiculous situation of performing RCTs of interventions with as much scientific plausibility as a Harry Potter spell. By which I mean homeopathy, acupuncture, osteopathic or chiropractic manipulations, aromatherapy, and any other quackery that you can think of.
Evidence-based medicine has sometimes become divorced from the scientific baseline that should underlie it all. When an intervention is tested that has no real prior plausibility, there is always a risk of a spurious positive result just from random effects. Add to that the fact that, very often, investigations of unscientific interventions are often designed and performed by “true believers”, leading to methodology and interpretation biases. Positive trials can then be interpreted as proving that an intervention which cannot possibly work has actually been shown to be effective.
There are a few recent examples in neonatology of unscientific nonsensical interventions being published as showing that they are effective. Fortunately, I don’t think that applies to homeopathy, at least, I just did a search of Pubmed for randomized trial of homeopathy in the newborn and I found nothing from an NICU, although there were a couple of trials in older children. For anyone not aware, homeopathy requires the administration of enormously diluted substances, which, in their undiluted state, reproduce the symptoms of the disease being treated. Dilutions are usually so extreme that most often, when someone takes a homeopathic medication, they are not getting even a single molecule of the original substance. According to the nonsensical theories that underlie homeopathy this makes them more effective, the more diluted they are, the stronger the effect. Sometimes the medications that are actually sold as being homeopathic remedies do, in reality, contain active ingredients, which may be toxic. Death from atropine contamination of a supposed homeopathic teething remedy has been reported, and hundreds of adverse effects have been noted, which are, of course, not because truly homeopathic remedies are toxic, they are not, they are just water, but it is because some of what are sold as homeopathic remedies actually contain toxins.
Acupuncture is just as unscientific as homeopathy, being based on ideas about a life force (Qi, a very useful word if you are playing Scrabble, but not a scientific concept) which is conducted in meridians. Neither Qi nor the meridians actually exist. There are many RCTs of acupuncture in the literature, and objective evaluations have shown that the better the controls the less the efficacy of acupuncture, for any outcome. Controlled trials have shown that it doesn’t matter where you put the needles, or even if the needles actually puncture the skin. Acupuncture is most often studied as an analgesic, and is sometimes “enhanced” by passing an electrical current between the needles, this is often touted as being a variety of acupuncture, but is actually a variety of TENS. In other words, acupuncture is just a theatrical placebo, and one we should not subject our patients to, it has zero prior plausibility, given the lack of any scientific evidence for the existence of Qi, or the existence of meridians.
It is indeed unfortunate that otherwise sensible physicians can be misled into performing research studies of this nonsense, it becomes a despicable failure when they are performing painful procedures on babies and not giving them appropriate analgesia. The supposed justification for this “research” is that acupuncture is used a lot, even in children, and some studies seem to show analgesia. But, as I already mentioned, the apparent effect of acupuncture on pain gradually becomes less as the studies are better designed.
The most recent investigation of quackupuncture that I saw from an NICU was an investigation of what is called laser acupuncture! (Stadler J, et al. Laser acupuncture versus oral glucose administration for pain prevention in term neonates. Acupunct Med. 2021). That is, shining a light on the skin of the baby, which was supposed to be worth investigating as analgesia prior to heel pokes. But wait, they used the quackupuncture point LI4, which is well known to be the magical non-existent point, “Large Intestine 4” so what could go wrong? What went wrong of course was that the intervention was not blinded (although the person evaluating the videos of the babies responses to the heel poke was supposedly masked) the control intervention was “30% glucose solution over a period of 30 seconds”, but no dose is noted, there is no mention of soother or swaddling or skin-to-skin contact, all of which are effective in markedly reducing pain responses to heel pokes. The PIPP scores increased to a median of 12 in each group, which shows there was inadequate analgesia in both groups. PIPP scores over 7 imply that the pain is substantial, and good analgesic approaches, with swaddling and sucrose and a soother, or with kangaroo care, for example, will usually maintain PIPP scores less than 8, in this study for example, with a higher dose of 0.5 mL of sucrose the median PIPP score was 5 during the procedure, compared to 7 with the lower dose of 0.2 mL. In another study the effects of kangaroo care and sucrose were shown to be equivalent, and the median PIPP score hardly changed across the study, with a median of around 6.
The result of the Stadler et al trial, therefore, showed that acupuncture was basically useless, and so was the control intervention. Of course, as they usually will, the believers in acupuncture try to find some signal in the noise to pretend that maybe shining a light on the babies skin did indeed have an analgesic effect, and they come up with the observation that the heart rate slowed down faster after the laser light “therapy” than after inadequate glucose therapy.
What about ear acupuncture? Well, just as ridiculous as the above trial, is an investigation of sticking magnets to the babies ear, which is touted as being a safer form of TCM (Traditional Chinese Medicine). (Gan KML, et al. Magnetic Non-invasive Auricular Acupuncture During Eye-Exam for Retinopathy of Prematurity in Preterm Infants: A Multicentre Randomized Controlled Trial. Front Pediatr. 2020) Ear acupuncture actually has nothing to do with TCM, it was invented in 1957 by a French physician, Paul Nogier, who thought that the folds in the outer ear resembled a fetus, so he thought that sticking a needle in the stomach of the “fetus” would be good for stomachache. Since then, other points have been made up, which are supposed to represent specific parts of the brain. Because, I guess, people shied away from sticking needles in the ears of the babies, they decided to glue tiny magnets to them instead, the justification given for this, in a previous article, was that magnetic fields have been shown to have biologic effects. Which is true, but the review article they gave as a reference refers to fields up to 8 Tesla! Which is about 8 times more than an MRI and about a trillion times more than the tiny beads that they stuck on the babies ears. And even if there were some measurable effect on blood flow in the skin under the magnetic bead (for example), so what?
The beads were actually moved around the ear, in a procedure laughably called “Battlefield acupuncture”! Supposedly, the name is derived from use in the battlefield of medical practice, and the myth has grown up that it is used by quackupuncturists for acute pain from injuries. The magnetic beads are moved around the ear sequentially, to points which have been invented to represent: (1) Cingulate Gyrus, (2) Thalamus, (3) Shenmen, (4) Cranial Nerve-5 (Ophthalmic branch). This reminds me of witchcraft, casting spells using nonsensical words designed to impress. In this particular case the magic spell was invented in 2001, and the evidence for its efficacy, according to the practitioner that invented it, is that people attending the inventor’s course give him laudatory comments! Who needs science when you have evidence like that! I wonder if, like magic spells, if the beads are moved around in the wrong order, or backwards, then that reverses the effects and may cause mayhem!
Why anyone with a training in medical science would give any credence to this nonsense is beyond me, still less to organise a multi-centre trial of sticking magnets to the ear for pain relief during retinopathy screening. Nevertheless, that happened, and the trivial differences in PIPP scores between the groups, (which are presented as mean and SD, even though this is an ordinal scale) were means of 13.5 and 11.9, with SD of around 4 in each group. The results are actually presented with an incomprehensible table which includes the value of something called the “intercept” and seems to show that the baseline scores were also different between groups, by 0.7.
But doesn’t the “significant” p-value mean that the authors showed an effect, you might ask? Let us for the moment assume (and it is a very big assumption) that the analysis of the videos was indeed completely masked to study group. As mentioned above, the people doing the trial are clearly “true believers”, so it would be completely unsurprising if there had been some “leakage” of information, with some degree of partial unblinding. The person who applied the stickers was unmasked, which scould easily have some impact on the proceedings.
The prior probability of the analgesic efficacy of moving tiny sticky magnets around various made-up spots in the ear is about as close to 0 as it is possible to be; but let us be generous and propose that there is a 0.01% chance that sticking tiny magnets to the ears of preterm babies could affect pain responses, by some undescribed mechanism, dependent on unknown biochemical, cellular, and anatomical pathways. In that case, using Bayesian reasoning, even with a p-value of 0.03, it remains incredibly unlikely that the finding represents a real phenomenon.
I think it is shameful that this study was performed. It is shameful that the ethics review committees of these hospitals approved this study, the Royal Hospital for Women, Sydney, the Royal Alexandra Hospital, Edmonton, and the University Malaya Medical Center, Kuala Lumpur, have a lot to answer for, research is only ethically acceptable if it is scientifically valid. Wasting the resources involved in performing this study, and impacting the lives of the families who consented is shameful. Frontiers in Pediatrics should be ashamed to have published it.
Adequate pain relief for retinopathy screening is a major problem for our patients, and we really need to investigate science-based methods to reduce they distress they experience.
It can sometimes take years for major advances in medicine, based on clear evidence of improved outcomes, to lead to shifts in practice. One example is the initial demonstration by Liggins and Howie that antenatal steroids (ANS) improved survival of preterm infants, it took 23 years before the American College of OB/GYN supported their use, and low rates of ANS treatment are evident in the data from trials (that is, even from active academic centres) well into the 1990’s. Sometimes the opposite happens, there is a huge shift in practice, even affecting patients for whom there is no good evidence, when the advantages are questionable, and adverse effects have not yet been ruled out.
Perhaps because of their tardiness in accepting ANS prior to very preterm delivery, our US Obstetric colleagues seem extremely keen to use ANS prior to late term delivery. Remember that, in the pivotal ALPS trial (Antenatal Late Preterm Steroids) although “statistically significant”, there was a relatively modest impact on the primary adverse outcome (death or respiratory disease needing over 30% oxygen or positive pressure), an absolute 3% reduction, which was mostly due to an absolute 3% reduction in need for CPAP/Highflow cannula; there were no deaths in either group. That trial also showed an absolute 3% decrease in NICU admission, and an absolute 9% increase in hypoglycaemia, with an NNT of 33 to prevent an additional baby needing CPAP, and an NNH of 11 to have one more baby developing hypoglycaemia.
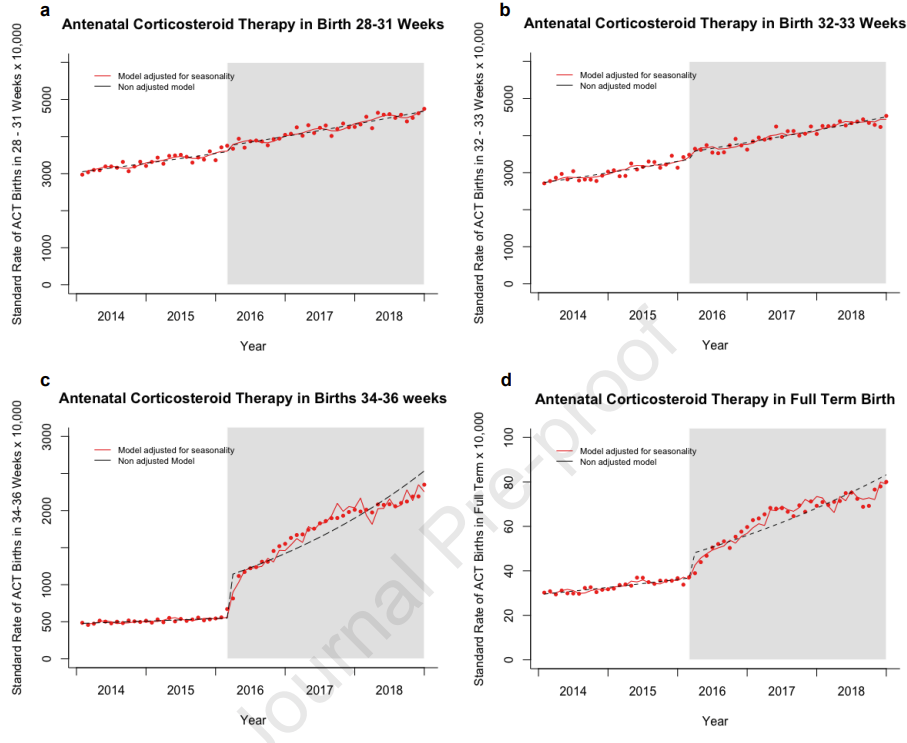
This new publication demonstrates how much ANS prior to late preterm delivery has changed since then, and the “spill-over” into use for deliveries at term.
These data from a birth certificate database show an immediate dramatic increase in ANS usage, and ongoing increases in use since then, with the shaded part of the graphs starting in Feb 2016 when the trial was published in the NEJM.
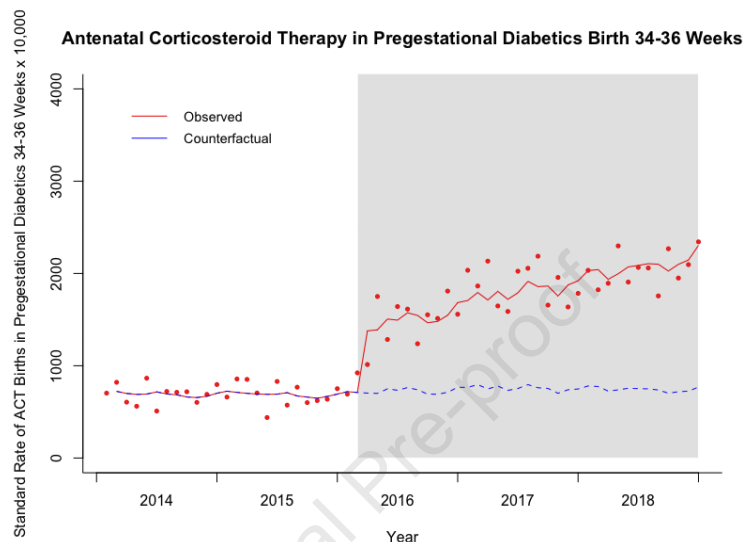
Women with diabetes diagnosed prior to pregnancy were not eligible for the ALPS trial, but that hasn’t prevented a major increase in use of ANS for those women, prior to late preterm delivery. The trial also excluded women presenting at full term.
It is really unclear whether ANS are safe for this group of mothers and babies, despite what I said recently about hypoglycaemia, I don’t think we should be trying to create more of it! Particularly among mothers who would not have been eligible for ALPS (term or diabetic) the risk/benefit ratio is completely unknown.
Why ANS might increase hypoglycaemia is studied in another on-line first article in the same journal (Battarbee AN, et al. Mechanism of neonatal hypoglycemia after late preterm steroids: are fetal metabolic effects responsible? Am J Obstet Gynecol. 2022). One would guess that it might be due to endocrine effects, and specifically that betamethasone, which obviously crosses the placenta and has potent glucocorticoid effects in the foetus (that’s why it is being given), would lead to foetal hyperglycaemia and to downstream secondary hyperinsulinaemia. Which is what this study was examining. It was an analysis of data from a subset of babies in the ALPS trial who had umbilical cord blood stored; C-peptide, insulin, leptin, and insulin-like growth factor binding protein 1 (IGFBP-1) were measured in just over 200 babies, about 30% of whom developed hypoglycaemia, 33% in the ANS group and 27% of the controls. The C-peptide, insulin and leptin levels were higher in the ANS babies, and were strongly associated with hypoglycaemia, especially high insulin concentrations above the 90th percentile which had an Odds Ratio for hypoglycaemia of over 6.0.
Should we be giving ANS prior to expected or planned late preterm deliveries? There have been a number of concerns cited and, despite my snide comments about the ACOG earlier on, the current advice regarding late preterm ANS is well written and discusses the potential risks in detail, with a helpful “summary of Evidence” table in an appendix. I must say I disagree with their final conclusion, which is “We recommend offering a single course of antenatal corticosteroids (2 doses of 12 mg of intramuscular betamethasone 24 h apart) to patients who meet the inclusion criteria of the ALPS trial, ie, those with a singleton pregnancy between 34 0/7 and 36 6/7 weeks of gestation who are at high risk of preterm birth within the next 7 d and before 37 weeks of gestation”. They do also recommend, within the document, “against the use of late preterm corticosteroids in pregnant patients with pregestational diabetes mellitus, given the risk of worsening neonatal hypoglycemia”, although the increase in neonatal hypoglycaemia was demonstrated in the ALPS trial which excluded mothers with pregestational diabetes, and therefore applies to all the newborns who are exposed. They have a reasonable discussion of the potential adverse impacts on brain development and they “recommend that patients at risk of late preterm delivery be thoroughly counseled regarding the potential risks and benefits of antenatal corticosteroid administration and be advised that the long-term risks remain uncertain”.
How many obstetricians are really equipped to thoroughly counsel expectant mothers about the possible adverse impact of ANS prior to late preterm birth and the uncertainty of the scientific evidence? How many mothers are equipped to understand and make an informed choice? If I were in that situation (easy to say for someone who could never have been) I would just about be able to comprehend the data and the implications of the data, and that is with a subspecialty in neonatology and years perusing the literature! Perhaps ACOG, and their society for maternal fetal medicine who authored the guidelines, could produce a YouTube video for parents that summarizes the information in a way that most could understand.
If you examine the data from ALPS in detail (the online supplementary appendix) you find that there was no advantage to ANS if the woman was randomized at or after 36 weeks, there was exactly the same incidence of the primary outcome, 7.1%.
The benefit of the steroids was much greater with planned cesarean; 26% primary outcome in controls reduced to 16% with steroids, compared to planned vaginal delivery where the difference was 12.4% to 10.7%. The benefits were also much greater in the group with indicated preterm delivery (induction or cesarean), compared to preterm labour or ruptured membranes, below are the numbers and percentage of the adverse primary outcome according to indication, from the supplementary appendix, the first column of results being the betamethasone group, the second being control, the 3rd is the relative risk and compatibility intervals, and the final figure being the interaction p-value.
You can see that the absolute reduction in the primary outcome is about 1.5% for the first 2 indications, and about 4% for those with induced labour or planned cesarean deliveries.
The ACOG statement reviews some of the evidence suggesting a possibility of long term impacts on brain development, and comes to no clear conclusion as to whether this intervention is safe or not, which I think is the correct interpretation, there is no clear conclusion.
As I said above, I disagree with their final conclusion that ANS should be offered to all women with increased risk of preterm delivery at 34 to 36 6/7 weeks. The evidence of benefit at 36 weeks is lacking, and those babies are just being exposed to an increase in hypoglycaemia and the unknown long-term effects without a benefit. The benefits are also quite small in ruptured membranes or preterm labour, with an NNT of about 67, and that should be taken into account in the decision making.
Nevertheless, there has been widespread uptake of ANS prior to late preterm delivery, hopefully there will be good long term follow up of the babies in ALPS, that is the only way we will tell in the future whether this major change in practice is actually improving outcomes for babies, or not.
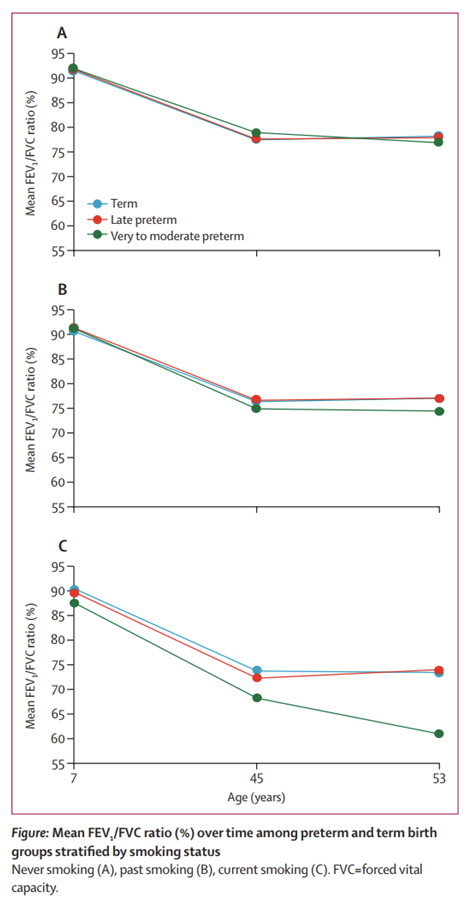
One of the most addictive and harmful drugs of all is perfectly legal. Tobacco, and the nicotine it contains, are subject to prohibition for adults nowhere in the world, despite millions of deaths, prolonged severe disability, and being probably as addictive as cocaine or heroin. We have long thought that the lung injury that preterm babies experience will probably lead to worse outcomes in adulthood, with a chance of increased COPD, this study tests that belief. (Bui DS, et al. Association between very to moderate preterm births, lung function deficits, and COPD at age 53 years: analysis of a prospective cohort study. The Lancet Respiratory Medicine. 2022). In fact, overall, the results from this study of follow up at 53 years of age are quite encouraging. Although there were very few of the very preterm babies, 28 to <32 weeks, (there weren’t many survivors less than 32 weeks in 1961) when added with the moderate preterm, 32 to <34 weeks they had a cohort of 46 babies to compare with over 1400 full term infants, and 172 late preterms.
The post-bronchodilator forced expiratory flows were a bit lower in the very to moderately preterm-born subjects, but only among those who also smoked. The non-smokers look identical between the preterm and the term born subjects.
Our current NICU survivors, who often have chronic lung disease, will probably have a very different profile in their long term than the babies in this study, we can imagine the potentially horrific effects of cigarette smoke on their pulmonary function in late adulthood.
Assuring good long-term health of former preterms looks like it will be critically dependent on finding ways to stop them smoking. Perhaps the proposed ban in New Zealand, which, starting in 2027 will make it illegal to supply cigarettes to anyone born after 2008, is the way to go. I think we should probably start sooner than that, and, as we know that parental smoking is a strong predictor of whether their children start smoking, stopping-smoking interventions for parents of preterms should be a priority.
A great deal of time and effort is expended to detect and treat low blood sugars in the newborn. Studies to determine risk factors, monitoring schedules, and treatment strategies have taken a great deal of effort, and implementing the recommended protocols requires much effort, resources, and often separates healthy babies from their families, or at least makes them think the baby is sick. The whole point of all this is to prevent brain injury from hypoglycaemia, with the underlying premise that low blood sugars, below a certain threshold, may cause damage which will have an impact on the baby’s future, therefore it is important to detect and immediately treat the phenomenon.
Two new publications from studies co-ordinated by the Auckland group continue to challenge some of our assumptions.
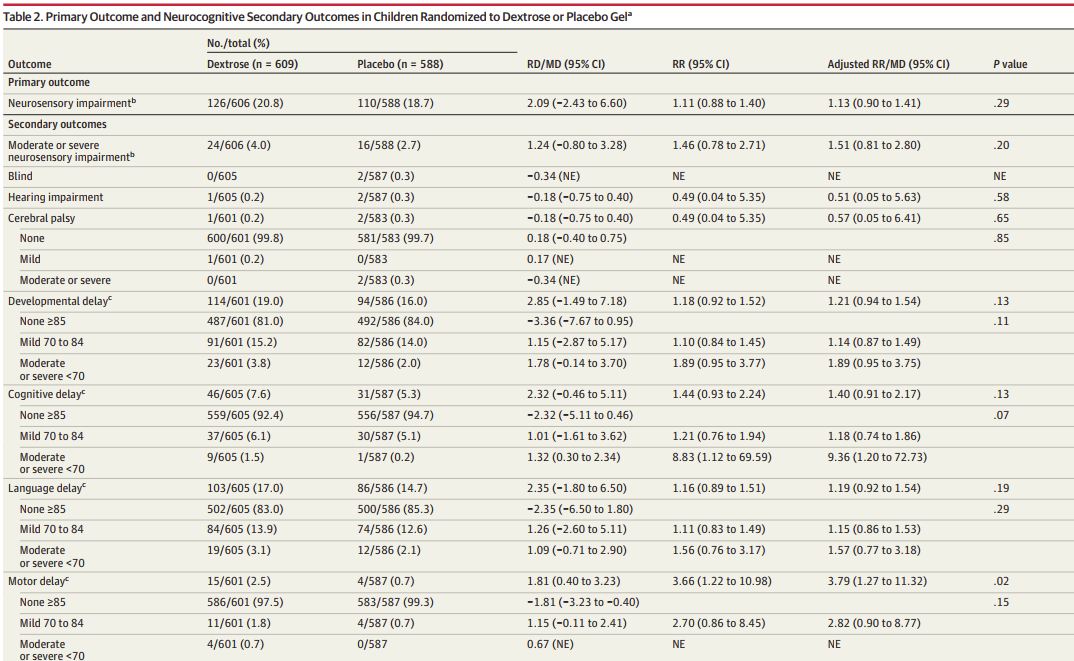
The small differences in outcome are all in favour of the placebo group. With, in particular, motor delay being more common in the dextrose group, 2.5% compared to 0.7%.
The average scores on each composite of the BayleyIII scores were higher in the placebo group, and, although the differences were very small, some of the 95% compatibility intervals for the unadjusted and adjusted mean differences did not include 0.
There were also tests of executive function which showed practically identical results in the 2 groups. On other words, no advantage at all, and some hints of an adverse impact of the oral gel when used as prophylaxis.
The other publication is from the CHYLD team, (Shah R, et al. Association of Neonatal Hypoglycemia With Academic Performance in Mid-Childhood. JAMA. 2022;327(12):1158-70). This is an evaluation of academic achievement in 480 infants from a prospective cohort, at 9 to 10 years after enrolment, which is 82% of the potentially eligible children. The children had initially been participants in either the BABIES study or SUGAR-BABIES: BABIES was a prospective cohort study of EEG monitoring in neonates at risk of hypoglycaemia, which showed no impact of hypoglycaemia on EEG activity; SUGAR-BABIES was the randomized trial of oral glucose gel as treatment for hypoglycaemia, which showed that the intervention was effective as treatment. Previous publications at 2 years showed no apparent impact of hypoglycaemia, whereas at 4.5 years there was some evidence of an association between hypoglycaemia and poor executive function. To recall in the 4.5 year follow up there were no differences in neurological outcomes or on Wechsler full scale IQ, and mean executive function scores were practically identical in the 2 groups, 13.5 (SD 6) compared to 13.3 (SD 5.7), but there was an excess of babies with scores more than 1.5 SD below the mean, 11% vs 5%, suggesting a slightly skewed distribution with an excess of lower scores in the hypoglycaemic group.
These 4.5 year findings reinforced the importance of performing this new evaluation at 9 to 10 years. Academic achievement, executive function, visual-motor integration, motor function, visual processing and behavioural problems were evaluated. No differences were found between infants with hypoglycaemia (either one blood glucose <2.6 mM/L (47 mg/dl) or an interstitial glucose <2.6 for over 10 minutes) and those who never had documented hypoglycaemia.
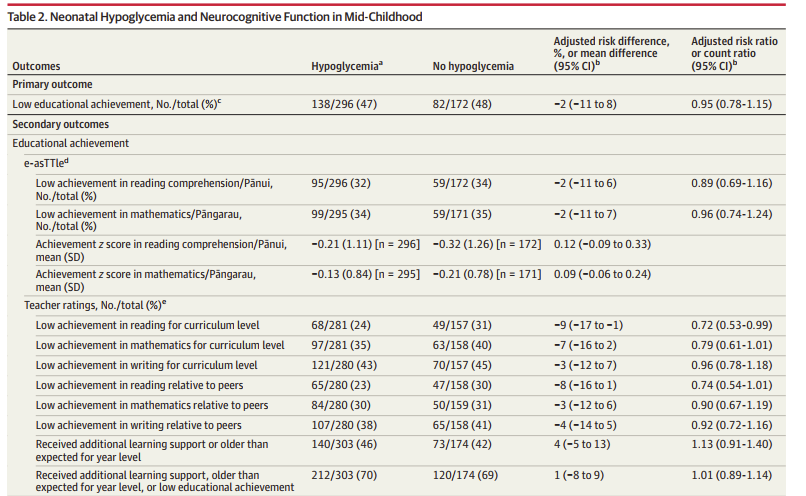
The differences in outcomes were small, with minor differences generally favouring the hypoglycaemia group, the only outcome for which compatibility intervals did not include no difference was the teachers evaluation of reading ability, that also favoured the hypoglycaemia children. They also evaluated the subgroup with severe (<2.0 mM/L (37 mg/dl)) or recurrent (3 or more) hypoglycaemia, and the subgroup with recurrent hypoglycaemia (3 or more episodes). None of the results look different from non-hypoglycaemic children. Here is the first part of the first results table:
What is somewhat surprising, is how frequent low educational achievement was in all of the groups, with almost half of all the participants being “below the normative curriculum level” or “well below”, below seems to mean that they were operating at a level at least 1 year behind their peers, and well below means more than 2 years behind. This isn’t totally clear in the publication, but the statistical analysis plan in the supplement defines “below” as performing at a level 4 to 7 school terms below the peer group and, according to Google, each school year in New Zealand consists of 4 terms. “Well below” is defined as performing at a level 8 or more terms behind the school year and term norms.
The power calculations were based on the prediction that 20% of children would have this outcome. Poor educational achievement was therefore very frequent in all groups, and more than twice as frequent as expected, even though achievement was not affected by whether the children had actually developed hypoglycaemia or not.
It seems therefore likely, that the same factors that lead to an increase in risk of hypoglycaemia also lead to an increased risk of poor academic performance, and also poor outcomes in visual-motor integration, executive function and behavioural domains. These findings emphasize the need for control groups in studies of long term potential impacts of hypoglycaemia to be babies with the same profile of risk factors, but who did not develop hypoglycaemia. That has not always been the case and may have misled us as to the importance of hypoglycaemia. Obviously, if you compare at-risk babies who develop hypoglycaemia to the general population, then they would seem to have much worse outcomes. It appears that being small for gestational age or an infant of a diabetic mother, and late preterm birth are risk factors for poor outcomes on the variables that were studied. There is also a question about the background frequency of social deprivation, and the population appears a little more deprived than the general NZ population, with about 40% of the participants’ families being in the most deprived 3 deciles (it should of course be 30%), but that doesn’t to seem to me to be a big enough finding to explain most of the results.
The most dramatic interpretation of these data would be that hypoglycaemia, to <2.6 or even <2.0 mM/l is unimportant in the transitional period. Single episodes or even multiple episodes below these thresholds don’t seem to increase risk of poor outcomes, over and above just being in an at-risk group. One possible explanation of the results could have been that we miss a lot of hypoglycaemia events, and the poor outcomes might be due to undetected hypoglycaemia. However, many of the children in CHYLD had continuous interstitial glucose measurements performed and the analysis, presented in the supplement, of only babies with continuous monitoring also showed that babies who were continuously normo-glycaemic had identical poor outcomes to those with documented hypoglycaemia, and to those with hypoglycaemia during their continuous monitoring period, 48% of normo-glycaemic infants having poor educational achievement.
These data suggest that we should maybe focus on detecting and treating more severe and prolonged hypoglycaemia. It has already been shown that using 2.0 as a limit rather than 2.6 mM/l (36 rather than 47 mg/dl) does not affect long term outcomes, these new data imply that even 2.0 is too high a threshold, using dextrose gel as prophylaxis actually slightly worsened outcomes compared to placebo, and babies with documented hypoglycaemia actually did slightly better than normoglycaemic infants.
Could it be that all our screening and interventions for mild and moderate hypoglycaemia in term and near term babies are actually making things worse? Is there any way of predicting which babies are at risk of more severe hypoglycaemia? What threshold of hypoglycaemia is associated with worse outcomes? Does treating hypoglycaemia when it fall below that threshold improve outcomes? Is it possible to focus prophylaxis to prevent more severe hypoglycaemia? If so, does that improve outcomes?
And for our obstetric colleagues, can we prevent gestational diabetes, intra-uterine growth restriction, excessive intra-uterine growth, and late preterm delivery? If so, does that improve long term outcomes of these babies?