
The title is deliberately a bit vague as I wanted to discuss whether GOR contributes to the pathogenesis of BPD, and also whether it is important in infants with established BPD.
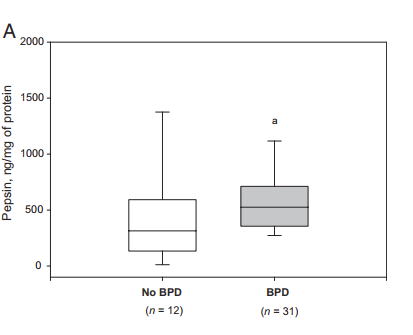
Does GOR contribute to the development of BPD? There is so little reliable data to answer this question that I can only offer the old Scottish verdict of “not proven”. It is a possibility that GOR and aspiration of refluxed intestinal contents could contribute to lung inflammation and damage. I don’t think it would be too difficult to prove, actually, intubated infants could have recurrent endotracheal aspirates examined for pepsin (which should ordinarily not be in the lungs) and a correlation between evidence of aspiration and the development of lung injury. As far as I know, this has only been done once, (Farhath S, et al. Pepsin, a Marker of Gastric Contents, Is Increased in Tracheal Aspirates From Preterm Infants Who Develop Bronchopulmonary Dysplasia. Pediatrics. 2008;121(2):e253-9) with a rather unconvincing increase in pepsin concentrations among infants who developed BPD compared to those without BPD. You can see the figure below, and although the difference is “statistically significant” it doesn’t look very useful with a major overlap between cases and controls. Of note, 92% of their samples (and all of the babies at least once) were positive for pepsin, suggesting that micro-aspiration is universal, the results suggest that perhaps that having a bit more pepsin in the lungs increases lung injury (at least using oxygen at 36 weeks as the indicator of lung injury).
Apart from that study I can find no real evidence that suggests that recurrent micro-aspiration is important in the pathogenesis of BPD. Even if we strongly suspected it to be true, the next question would be what to do about it? If the culprit were gastric acid, then gastric acid blockade should decrease BPD, but that has never been shown. If it was due to other enzymes and inflammatory responses then actually decreasing episodes of reflux should decrease BPD, but we don’t know how to do that. One observational study from a center which sometimes uses transpyloric feeds showed that those where the neonatologist decided to start transpyloric feeds in the first week of life had shorter duration of assisted ventilation and a little bit less “death or bpd” but there are major problems with this study design. Although the authors attribute this difference to reduced GOR and reduced aspiration, there is no evidence that transpyloric feeding in preterm infants actually decreases reflux. In a study in older children with transpyloric feeds, they all had at least one episode of reflux on impedance pH monitoring, and some had very frequent episodes despite receiving transpyloric feeds. Critically ill adults with transpyloric feeds almost all have reflux of duodenal contents into the stomach, and almost all have gastro-oesophageal reflux and pulmonary aspiration, with only minor differences to controls randomized to gastric feeding. The latest version of the Cochrane review of transpyloric feeding in the newborn notes an increase in mortality, more GI disturbances, no change in aspiration pneumonia/pneumonitis, no data on BPD, and an overall poor quality of available data.
Even if BPD were clearly more common among babies with recurrent micro-aspiration there is no evidence-based way to prevent, or even reduce, that phenomenon in the newborn.
But what about after lung injury has developed? Do babies with BPD have more reflux than those without? Does GOR adversely impact respiratory function or clinical progress in infants with BPD? Does treating reflux improve clinical outcomes in babies with established BPD?
In 1989 a publication compared acid reflux to the proximal oesophagus between preterm infants (on full feeds, at about term) with and without BPD. They actually found less reflux in the BPD infants. A more recent study from 2004 also using pH-metry found the same thing, less reflux among babies with BPD compared to controls of similar gestational and post-menstrual age without BPD. A 2015 study, using impedance as well as pH monitoring showed no difference in reflux events between BPD and control babies who all had “symptoms consistent with GOR”. That study was only able to find a difference after multiple quantile regression analysis, and only in pH-only events, that is, events which dd not show evidence of bulk fluid movement into the oesophagus.
I haven’t been able to find any reliable evidence to address the second and third questions, which are obviously linked. Even though GOR does not appear to be more common in babies with BPD compared to control preterm infants, it could still be associated with worse lung injury and babies could possibly benefit from treatment, and evidence of an adverse impact would be strongest if reducing GOR actually improved lung function. The big problem of course is the lack of effective treatments of GOR. Although commonly referred to as anti-reflux treatments, acid blockade with histamine receptor antagonists or proton pump inhibitors do not, of course, reduce reflux. Unless symptoms are only due to acidic GOR they will have no effect. There is no good evidence to support the use of any prokinetic agent, those that have been investigated are as likely to show an increase in reflux as a decrease.
The recent article about medication use in the NICU that I already discussed was somewhat reassuring that there had been a decrease in the use of lansoprazole between 2010 and 2018, (and of ranitidine, but that had been taken off the market). I couldn’t see much else on the list that is being used to replace them, there is rare use of famotidine and omeprazole. I was surprised to see both sucralfate and simethicone on the list of NICU drugs, which maybe are being given for perceived GOR symptoms, but simethicone doesn’t even work for colic, the usual indication, at least as according to the only placebo controlled RCT that was performed; Sucralfate is 21% aluminium by weight, so probably not a good idea to give to developing brains.
In summary then, there is no good evidence that GOR and microaspiration are important in the pathogenesis of BPD, there is no good evidence that infants with BPD have increased GOR compared to other preterm infants, and there is no good evidence that GOR has an impact on respiratory function in established BPD.
Even if, in an individual patient, you thought that GOR might be contributing to their pulmonary symptoms, I reiterate that there isn’t much you can do about it. There is no evidence-based effective medication that safely decreases GOR or GORD. Thickening feeds has a minor effect on reflux, but has never been shown to improve any clinical aspect of GORD. Transpyloric feeding does not eliminate GOR, and, in the only trial in infants with established BPD, transpyloric feeding seemed to increase hypoxic spells. All you can do is try and keep the babies upright especially after feeds (this might have no direct evidence base, but kangaroo care has many benefits, and gravity can be our friend), and wait for improvement.







Thank you for guys common sense review of a topic that often leads to confusion at the bedside!
I believe this publication was written by Keith Barrington, not Naveed Hussain
I don’t really understand the comment, Ted. Did I make a mistake? I’d be happy to correct if I’ve mis-attributed something.