
All babies have reflux, repeated transient lower oesophageal sphincter relaxations are universal. Almost all babies have overt regurgitation, I often say that if a baby never regurgitates it may be a sign that they aren’t getting enough milk!
So when does GOR become GORD? There are 3 groups of symptoms that are often ascribed to reflux in the NICU: apnoeas and recurrent bradycardias; respiratory deterioration/bronchopulmonary dysplasia; oesophagitis and resulting feeding problems.
There are many studies of the relation between GOR and either apnoeic or bradycardic spells. In order to have any idea of the reality of that relationship we need prolonged multichannel recordings which measure reflux objectively in addition to cardiorespiratory recordings which include airflow. In a study I did a few years ago now in San Diego we used pH recordings and found no relationship evident between apnoeic events and acid reflux. But, of course, most GOR in newborn infants is either neutral or alkaline, so its possible that we could have missed something.
Most of the available studies which have used impedance, and therefore detected non-acid reflux also, show no temporal relationship between episodes of reflux and acute respiratory events, some show that apnoea (particularly obstructive apnoea) may precede reflux events. There are one or two that have reported that acid reflux may trigger apnoeas in some infants, and a couple of studies, usually in small highly selected groups of babies, showing a temporal relationship between GOR events and obstructive apnoeas. One study, for example, in 7 former preterm infants around term found that among the 4 who had extremely frequent obstructive apnoeas (>6 per hour) there were 3 who seemed to have apnoeas preceded by GOR.
One interesting study from Jadcherla’s group in Columbus Ohio used the sort of intensive monitoring I have described, but with oesophageal manometry rather than impedance measures, and then introduced artificial pharyngeal stimulation with up to 0.5 mL of sterile water as a bolus. They found that overall former preterm babies who were evaluated at 36 to 40 weeks PMA with or without recurrent bradycardia had very similar responses to pharyngeal stimulation. A subgroup of the babies had more severe bradycardia after stimulation, the definitions the authors used are rather weird as they are based on the resuscitation guidelines NRP and PALS, which are of course completely irrelevant for episodic bradycardias in otherwise stable infants. Nevertheless, this study does suggest that some babies are more sensitive to pharyngeal stimulation than others and may have more severe bradycardias, but these studies were performed after discharge home, at around term post-menstrual age, and therefore not necessarily relevant to apnoea in the NICU.

This remarkable image shows a reflux event, using overlaid data from oesophageal manometry in addition to multiple impedance (the white lines). The reflux event starts with a transient relaxation of the LES, lower oesophageal sphincter, and the progressive drop in impedance in a cephalad direction is the bolus of liquid climbing the oesophagus, followed by major increases in pressure which are swallowing movements in the pharynx and then the purple wave of increased pressure moving down the oesophagus to clear the reflux. In the interesting review article from which that image was taken (Badran EF, Jadcherla S. The enigma of gastroesophageal reflux disease among convalescing infants in the NICU: It is time to rethink. Int J Pediatr Adolesc Med. 2020;7(1):26-30). There are other images also which show an association between episodic symptoms preceding a reflux event.
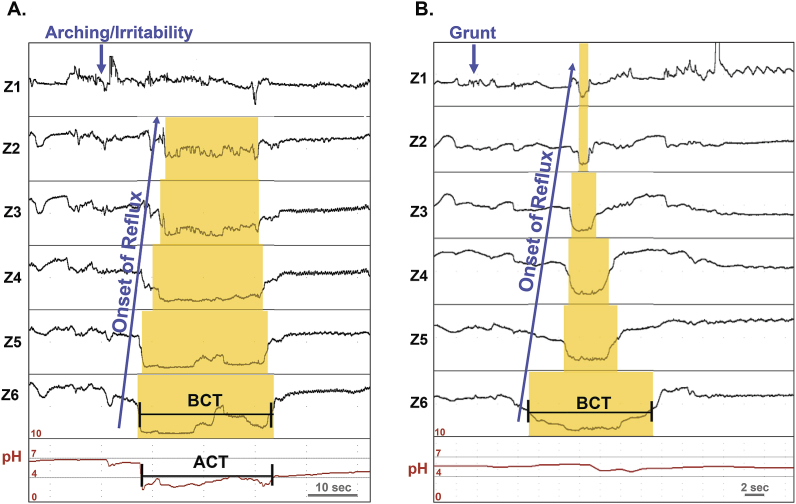
This looks to me as if the arching and irritability, or the grunt, caused the reflux, rather than the other way around! Indeed when symptom scores have been compared with objective recording of reflux in NICU patients, there has usually been no correlation. There are several studies that have almost all failed to show that symptoms ascribed to reflux are actually caused by reflux, four that I quickly found in my files are listed below.
I teach residents and fellows that the only clinical sign which is reliable for the presence of reflux is overt regurgitation. Even though reflux might sometimes cause clinical consequences (GORD) there is no way to determine its presence without prolonged impedance monitoring, which should be combined with pH and multi-channel recordings to have any confidence that clinical events are caused by reflux.
Also vitally important, most reflux in the newborn in the NICU is not acidic, and there is no evidence that the acidity of reflux episodes is associated with the likelihood of a reflux episode causing a clinical event. Using acid blocking medications therefore has no rational basis in the treatment of GORD if the justification for treatment is the presence of episodic cardiorespiratory events. And probably not for other possible respiratory indications either, a subject to which I shall return.
Funderburk A, et al. Temporal Association Between Reflux-like Behaviors and Gastroesophageal Reflux in Preterm and Term Infants. J Pediatr Gastroenterol Nutr. 2016;62(4):556-61. Snel A, et al. Behavior and gastroesophageal reflux in the premature neonate. J Pediatr Gastroenterol Nutr. 2000;30(1):18-21. Kohelet D, et al. Esophageal pH study and symptomatology of gastroesophageal reflux in newborn infants. Am J Perinatol. 2004;21(2):85-91. Mousa H, et al. Testing the association between gastroesophageal reflux and apnea in infants. J Pediatr Gastroenterol Nutr. 2005;41(2):169-77.







Thank you for covering this Keith. It was a really interesting summary of reflux, which we often struggle to know if and how to manage on our neonatal unit. What is your opinion on the use of feed thickeners in preterm infants who either appear to reflux or have recurrent apnoeas or bradycardias?
I don’t think there is any reason to treat apnoeas or bradys with anti-reflux measures. Specifically with respect to feed thickening there is no evidence whatever that they will decrease respiratory pauses, and very little evidence that they improve reflux! In older infants a systematic review found evidence of a minor effect on the duration of reflux episodes, no effect on the number of episodes and there is no data on the kind of baby we see in the NICU of preterm babies approaching term. Even the centre in Italy that finds more association between reflux and apnoea than most other investigators have not found any impact of thickeners on reflux or on apnoea. Corvaglia L, et al. Lack of efficacy of a starch-thickened preterm formula on gastro-oesophageal reflux in preterm infants: a pilot study. J Matern Fetal Neonatal Med. 2012;25(12):2735-8. Corvaglia L, et al. A Thickened Formula Does Not Reduce Apneas Related to Gastroesophageal Reflux in Preterm Infants. Neonatology. 2013;103(2):98-102.
In addition some thickeners have been associated with NEC. (mostly xanthan gum, I believe)
Overall, I would say that in an infant who has problematic reflux at term, non-xanthan gum thickening might slightly reduce the duration of reflux episodes, and might be worth a therapeutic trial, but, as reflux tends to spontaneously improve, a trial of stopping the thickener after a week or so is worth considering also.