
Human breast milk, when freshly expressed, contains all sorts of goodies, to use the technical scientific term. Many of which are adversely affected by standard pasteurisation (called Holder pasteurisation, which is very similar to what Louis Pasteur himself invented in the 1860’s). Holder pasteurisation entails heating the milk to about 63o Celsius and holding it there for 30 minutes, as far as I can tell, it is called the Holder method because of the process of “holding” the temperature stable for a period, but if that is wrong and someone called Holder should be credited I would like to know. I believe it is the only method used in human milk banks that follow HMBANA standards (or NICE standards or others internationally), even though it is no longer used much in the dairy industry, who use short term high temperature (72o for 15 seconds, or even for 5 seconds) processing instead. Other methods, including Ultra-High Temperature, high pressure processing, ultraviolet, and radiation treatments, can inactivate bacteria and other micro-organisms.
Holder pasteurisation has major effects on large molecules and less effect on small molecules (to over-simplify). So not much impact on oligosaccharides in general, but major decreases in immunoglobulins, various enzymes (e.g. lactoferrin), and larger hormones (adiponectin). Even some smaller molecules, such as insulin, are heat-labile and severely reduced by pasteurisation.
Occasional neonatal sepsis from bacterial organisms found in non-pasteurised maternal breast milk can occur, and even pasteurisation doesn’t kill everything, in particular spore-bearing organisms are resistant, which is why pasteurised milk is not the same as sterilised milk. Indeed contamination of pasteurised donor milk with Bacillus Cereus is a major reason for disposing of donated milk after pasteurisation, as it cannot safely be given to extremely preterm babies. In one recent study, the only culture positive organism after pasteurisation was B. cereus.
All forms of pasteurization, however, inactivate cytomegalovirus, and CMV from unpasteurized maternal milk is the major source of postnatal CMV infection in our patients.
There have been several publications recently about the importance of postnatal CMV acquisition in very and extremely preterm infants, the results of which are somewhat variable. I thought I would try to summarize what these recent publications tell us.
The most recent article is from Melbourne (Bimboese P, et al. Postnatal Cytomegalovirus Infection of Preterm and Very-low-birth-weight Infants Through Maternal Breast Milk: Does It Matter? Pediatr Infect Dis J. 2022;41(4):343-51) they followed very preterm (<32 wk) and/or very low birth weight (<1250g) infants of mothers who were CMV IgG positive. Just under half of the eligible mothers were antibody positive, and they were followed with breast milk and urine PCR for CMV. They eventually pared down the cohort to 58 babies, of 49 mothers, who were exposed to CMV PCR positive breast milk, and then compared the clinical course between those who became urine PCR positive, and those who stayed negative. The data are from around 20 years ago, for some reason, and at that time there was no human milk bank, so the babies received either fresh, refrigerated or frozen maternal breast milk, or formula, all of the babies received at least some fresh maternal BM.
“In total, 30% (8/27) of the CMV-positive infants were asymptomatic, 48% (13/27) mildly symptomatic, and 22% (6/27) severely symptomatic at the time of the first CMV-positive urine sample. Neutropenia was one of the most common presentations at the time of first CMV-positive urine (44%; 12/27), followed by respiratory deterioration (33%, 9/27; apnea (3), new CPAP requirement (1), new intubation (2), increasing oxygen requirement (7)). Nine of 27 infants had a partial or full septic workup”.
A much larger cohort of infants <1500 g birth weight was published in 2020, (Weimer KED, et al. Association of Adverse Hearing, Growth, and Discharge Age Outcomes With Postnatal Cytomegalovirus Infection in Infants With Very Low Birth Weight. JAMA Pediatr. 2020;174(2):133-40) from the Pediatrix group; because it is from a huge database the case definition and the comparison group are not quite as clear-cut, cases were defined by those who had a positive CMV culture or PCR from blood, urine, CSF, or respiratory secretions after 21 days. If they also had a positive test prior to 21 days they were classed as congenital, but if they never had a test before 21 days they were considered to have postnatally acquired CMV (and then analysed as a separate subgroup to see if that changed the conclusions). If a baby never had a CMV PCR or culture they were considered negative. The major outcomes of interest were: a failed hearing screen, length of hospitalisation and growth, with BPD and NEC being important secondary outcomes. Each of the 273 postnatally acquired CMV babies was propensity score matched with a control. Babies with postnatal CMV were much more likely to fail their hearing test, much more likely to develop BPD and there was very little NEC.
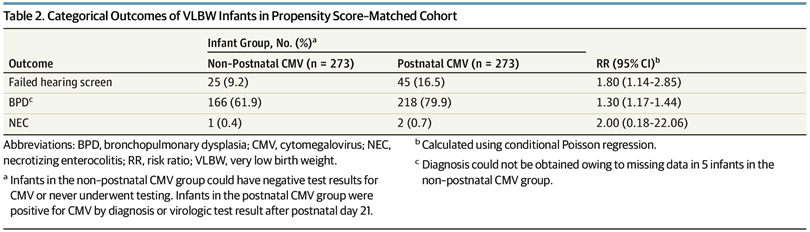
Length of stay was longer in the CMV babies, and there were some relatively small effects on weight growth, but not length or head circumference.
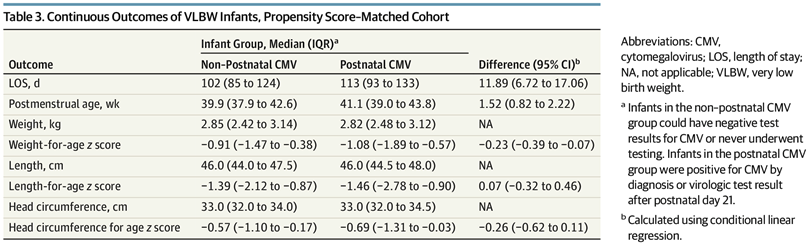
Remember that in that study there would have been many babies who never had a CMV pcr, so the overall rate of breast milk CMV transmission cannot be calculated.
A systematic review from 2021 (Park HW, et al. Incidence of Postnatal CMV Infection among Breastfed Preterm Infants: a Systematic Review and Meta-analysis. J Korean Med Sci. 2021;36(12):e84) suggests that among preterm babies of seropositive mothers, who receive breast milk known to be contaminated with the virus, somewhere between 2% and 87% will be infected. That is such a huge range that the data seem to be of little value, but the review includes some very tiny studies with only one or two cases. If you pool all of the studies then approximately 20% of preterm babies who receive CMV positive milk will become infected. It looks from that review, that the groups with more immature babies might have a higher risk, but transmission rates are so variable, that is not certain. However, a small study limited to babies of 22 to 24 weeks gestation (Mehler K, et al. High Rate of Symptomatic Cytomegalovirus Infection in Extremely Low Gestational Age Preterm Infants of 22-24 Weeks’ Gestation after Transmission via Breast Milk. Neonatology. 2013;105(1):27-32) showed a 65% rate of acquisition of CMV in the most immature infants, more than half of whom failed their hearing screen.
It also looks like freezing breast milk does not routinely lead to a lower rate of transmission. I mention freezing as it has been shown to partially inactive the virus, and is used as a routine in some centres for that reason. It has long been known that the impact on CMV inactivation is only partial. One RCT, despite limited power, showed that freezing was probably ineffective to prevent CMV transmission (Omarsdottir S, et al. Cytomegalovirus infection and neonatal outcome in extremely preterm infants after freezing of maternal milk. Pediatr Infect Dis J. 2015;34(5):482-9).
In contrast, pasteurisation of breast milk reliably inactivates CMV, and it doesn’t seem to make any difference how you pasteurise. Even a very short time, 5 seconds at 62O, is partially effective, (Bapistella S, et al. Short-term Pasteurization of Breast Milk to Prevent Postnatal Cytomegalovirus Transmission in Very Preterm Infants. Clin Infect Dis. 2019;69(3):438-44) and in that study they were able to pasteurise the milk daily, starting on day 4 postnatally using a system in the NICU milk kitchen, or even at the bedside. In this study they included infants of mothers who were CMV IgG positive, and then tested breast milk weekly. Breast milk was pasteurised routinely before being given to the babies unless CMV cultures of the milk proved negative. They ended up with 87 VLBW or very preterm <32 wk babies at risk of catching CMV from the breast milk, only 2 actually became CMV positive among the babies who received the short term pasteurised milk, whereas they had a historical control group of 83 babies who received raw milk, of whom 17 became infected. Although unfortunately not a randomized trial, this is certainly suggestive that this simple bedside method of pasteurisation can reduce, but not eliminate breast milk CMV transmission. This method has less effect on some large molecules, such as growth factors, but it probably has a major impact on Bifidobacteria, which are universally present in breast milk, are important for neonatal gut colonization and metabolism of oligosaccharides, and we should try and preserve if possible. I don’t know if there is any way to inactivate CMV without killing Bifidobacteria, but, if not, it warrants an RCT to determine if, in very preterm babies receiving CMV positive breast milk, there is an overall advantage of pasteurization or not.
In more general terms there is already one RCT of routine pasteurization of breast milk, (Cossey V, et al. Pasteurization of Mother’s Own Milk for Preterm Infants Does Not Reduce the Incidence of Late-Onset Sepsis. Neonatology. 2012;103(3):170-6) which I have mentioned a couple of times, and showed a 50% higher incidence of sepsis in infants fed pasteurized milk compared to raw maternal breast milk (possibly a random effect). A similar study, but confined to CMV positive breast milk, and with a sample size powered to determine sepsis, as well as growth outcomes, would be valuable.
In summary, somewhere around a quarter of very preterm babies exposed to CMV positive breast milk become infected, and the most extremely preterm babies are at much higher risk. The acute infection often presents with thrombocytopaenia, and sometimes neutropaenia, a sepsis like syndrome, respiratory deterioration, and apnoea. Postnatal, breast-milk acquired CMV, also appears to substantially increase the risk of failing hearing screening, likely to mean a real increase in hearing impairment. Breast milk acquired CMV also probably increases the risk of BPD, and, with, much less convincing data, perhaps increases retinopathy and NEC. Whether routine screening of breast milk for CMV, and some sort of pasteurization in selected cases is warranted, effective and safe is unknown.
One unanswered question I have, which is one of the reasons that I was reviewing this literature, is what about steroids? I have seen babies have very serious systemic CMV after steroids were given , but I struggle to find data about the impacts of steroid use on CMV infections in the preterm. Are babies who receive steroids and CMV positive breast milk at increased risk of serious CMV infection? Should we modify our decision-making in babies from CMV IgG positive mothers? If anyone knows any data about the issue, please let me know in the comments. A pubmed search using what I thought were the right terms came up with nothing relevant, and when I took “newborn” out of the search I had over 2000 hits!






