
Many preterm babies receive boluses of normal saline, often during the first 24 hours when their blood pressure is lower than desired. I have 3 serious questions about this.
- Are they indicated?
- Do they work?
- Are there adverse effects?
- Do hypotensive newborn infants have low blood volume?
The rationale for giving a fluid bolus is that the infant may be hypovolaemic, if they are, then you really don’t want to start other therapies if you could simply correct the hypovolaemia. I have some sympathy with this idea, I certainly wouldn’t want to start an epinephrine infusion if all the baby needed was to have 10 mL/kg of saline. But what is the likelihood that a hypotensive very preterm baby may have a low blood volume? There are a couple of studies that have attempted to measure circulating blood volumes in preterm babies, neither show any correlation between volume and BP, or volume and the occurrence of hypotension. Both studies were performed before widespread use of delayed cord clamping, which is very likely to make the association even rarer.
Generally then, no; preterm babies with hypotension are unlikely to be hypovolaemic, and after DCC extremely unlikely to be hypovolaemic. Unless the baby had a cord prolapse, vasa praevia, or was unable to have DCC for some reason, I don’t think we should even consider hypovolaemia. It is a rare reason for babies to be hypotensive after birth.
What about sepsis?
This is a trickier issue, the haemodynamics of neonatal sepsis have not been studied in as much detail as I would like, there are a few studies, which have studied mostly infants with Gran-negative sepsis, who may develop shock from the haemodynamic responses to endotoxins, or as a result of systemic inflammation.
It has become a sort of gospel in treatment of sepsis in older patients that they need huge amounts of fluids, 60 ml/kg is often given before patients are considered fluid unresponsive, at which time inotropes may be added to their therapy (this is what the current CPS recommendations for sepsis treatment in children state). But more recent trials in adults with septic shock are casting doubt on this approach. Two new large RCTs (here and here) have shown no harm from a restrictive approach to fluid management compared to liberal fluids. Admittedly to be enrolled in those trial the adults had to have already received a litre of fluid, but that is an awful lot less than 60 mL/kg. An updated meta-analysis including those trials confirmed a lack of difference with liberal compared to restrictive fluid management. Indeed the only large RCT I am aware of in children with septic shock showed an increase in mortality with fluid boluses.
As there is no good data in babies with septic shock, I think that an initial bolus of 10 mL/kg is reasonable, but may not actually turn out to be a good idea, after that the approach should be based on improving overall perfusion if it is impaired, increasing BP, if it is low and associated with poor perfusion, and/or improving perfusion of vital regions. Overall haemodynamic evaluation with functional echo, and regional evaluation with NIRS might help, but that is about as evidence-based as one can get. I start steroids early in treatment of septic shock, although I don’t know for sure that is right, 2 to 6 hours after starting hydrocortisone at lowish dose (2-3 mg/kg/day) things are usually getting better.
2. Do fluid boluses increase BP?
To return to our hypotensive preterm without evidence of sepsis, there is very little evidence that boluses even increase blood pressure. With the knowledge that BP is likely to trend upward anyway, you can only really answer this question with an RCT, but to my knowledge there has never been an RCT of bolus vs no bolus in hypotensive preterms.
Years ago, I did a little before and after study where we gave 15 mL/kg of 5% albumin to hypotensive preterms, and showed that mean BP increased by a mean of 2 mmHg for about 20 minutes, before returning to baseline, echocardiography at the time showed an increase in left ventricular output, but not right ventricular output, which means, in preterm babies with an open PDA, that the only thing the boluses did was to increase ductal shunting without improving systemic flow.
There are a few other short term haemodynamic studies showing very similar findings, i.e. increase in ductal shunt, little or no effect on BP.
3. Are there adverse effects?
This new publication (Sehgal A, Gauli B. Changes in respiratory mechanics in response to crystalloid infusions in extremely premature infants. Am J Physiol Lung Cell Mol Physiol. 2023;325(6):L819-L25) is what triggered this blog post, Arvind Sehgal and Bishal Gauli from Monash in Melbourne, recorded dynamic pulmonary mechanics from the VN500 ventilator before, during and after administration of a crystalloid bolus that had been prescribed by the clinical team.
Ventilator setting remained the same in these babies <29 weeks who were on volume guarantee ventilation. So a change in dynamic lung compliance will lead to a change in peak inspiratory pressure if the baby’s efforts remain similar.
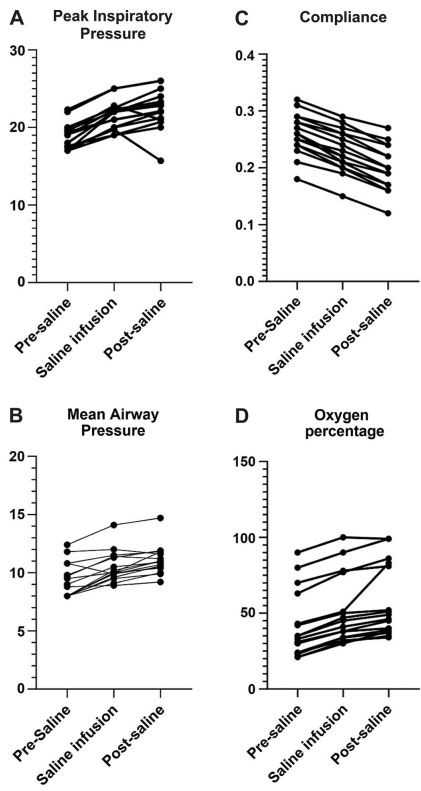
There was a trivial increase in BP with the boluses, 2 mmHg, which may well have been due to the variable nature of BP. As you can see, there was a worsening of dynamic compliance, leading to an increase in PIP, associated with an increase in FiO2.
The most likely explanation is an increase in pulmonary interstitial liquid, perhaps secondary to the increase in ductal shunting.
In view of the lack of evidence of hypovolaemia, the lack of response in BP, and the adverse effects, fluid boluses should generally be avoided in hypotensive preterm infants.







One – Seems a strange journal to choose for a clinical study in the NICU. Two – Perhaps I am misreading something but the methods are very confusing. For example, they downloaded continuously recorded data “60 min during the infusion” as one of the 3 time periods. The points on the graph representing that window are very discreet, so seems they represent one data point at one time. At the beginning of the 60m? The middle? the end? If average or median values from that time window, what about SD or 25/75 CI for each value? The Table gives median and IQR but how is that data derived? The median of all data points for all patients? Median based on each patient having one data point for each time period? If so, how was that data point derived. Would love more explanation.
Interesting read Sir. To be honest, this practice is a quite strange to me. If we are considering a newborn preterm with overt hypotension…including significant bradycardia… not responding to initial resuscitative measures … a bolus of normal saline even before epinephrine should be in order. Otherwise, as a routine?..quite strange.
The journal had ‘call for papers’ on PT respiratory physiology. Data point one reflects average of 30 minutes pre infusion data. Data point two reflects average of 60 minutes during the infusion and data point three reflects the average of data collected during 30 minutes post infusion