
As mentioned several times recently, artificial formula seems to lead to an increase in Necrotising Enterocolitis, compared to donor milk. Of note, the trials in the Cochrane Systematic Review include both those with the entire diet being formula or donor breast milk, as well as those where the infants were randomized to formula or donor milk as a supplement to their own mother’s milk.
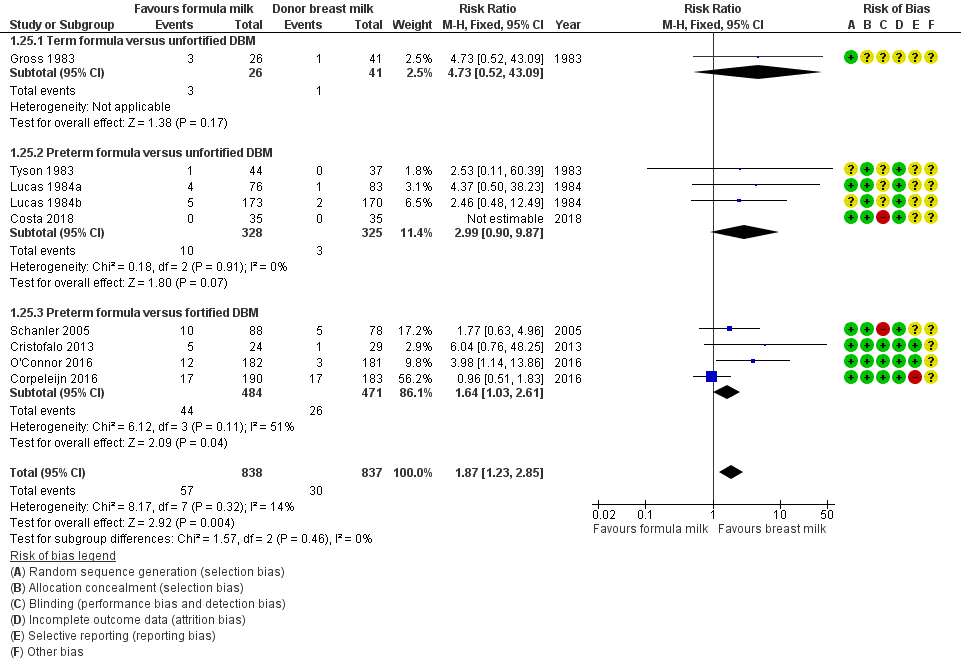
In the Forest plot from the Cochrane review, 3 of the 4 trials of “preterm formula versus fortified DBM” were among infants who had mother’s milk as the main diet, the entry criteria for Schanler 2005, Copeleijn 2016 and O’Connor 2016 included “mothers intended to breast feed”. The Corpelijn trial, however, only changed the diet for the first 10 days of hospitalisation, during which any supplement to mother’s own milk was either formula or un-fortified donor breast milk. In fact, I think there is an error in the classification of this trial in the Cochrane review, as far as I can see the babies in Corpelijn never received fortified donor milk; the babies received unfortified mother’s milk, which was supplemented either with artificial formula or unfortified donor milk until 10 days of age, after which they received maternal milk, with fortification according to local practice, and artificial formula as a supplement. The Cristofalo 2013 study only included babies whose mothers were not going to breast feed. Costa 2018 compared donor milk to artificial formula, but seems to have included babies whose mothers were not intending to breast feed, as well as those with insufficient milk. As a small study with no cases of NEC it is not informative for the NEC outcome in any case.
It is also useful to remember that the Schanler study had an extremely high frequency of NEC in the controls, and had nutritional practices which are not consistent with current best practice (“Administration of small quantities of MM (20 mL/kg per day) was initiated in the first week after birth and continued for 3 to 5 days before the volume was advanced. Milk intake was increased by 20 mL/kg daily to 100 mL/kg”), and it took an average of 18 days for the babies to receive even 50 mL/kg/day of milk. In contrast, in our NICU, similar babies of <1300 g (mean GA 27 semaines) achieved 150 mL/kg/day on average on day 16 with the previous version of our feeding protocol (it occurs now, with our progressive improvements in our feeding protocol, a little earlier).
Also, the Schanler 2005 study appears to have crossed over babies, and not analyzed them according to Intention to Treat: the methods include this phrase “Final group determination was made at the end of the study, on the basis of whether the participants had received the assigned supplement (Donor Milk or Preterm Formula)”. Which is very concerning, and raises doubts as to the reliability of the results.
In order to show whether there is an impact on NEC, therefore, you have to include data from the much older studies of Lucas. The reports of those trials are often a bit confusing as there was more than one trial running simultaneously, and the results are partly pooled, they included babies up to 36 weeks gestation, and had an enormous incidence of NEC among infants of 34 to 36 weeks gestation (9% if they received only formula, and 0/113 if they received at least some breast milk). It is unclear to me how relevant these data are to current practice, but one of those simultaneous trials was investigating donor milk or formula as a supplement to maternal breast milk. It was included in the Cochrane review as Lucas 1984b, which is the term I use in the figure below.
This is a Forest plot of the effects of supplementation of mother’s milk with donor human milk (Experimental) compared to artificial formula (Control) on the incidence of confirmed NEC. Lucas 1984b did not use the classification of Bell, but their “confirmed NEC” is similar to Bell stage 2 or 3.
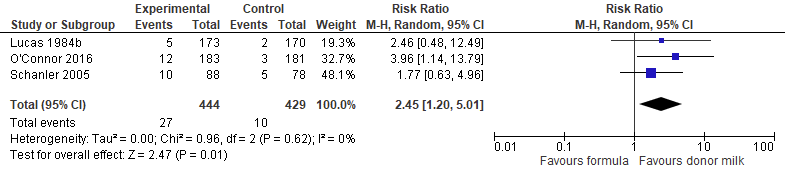
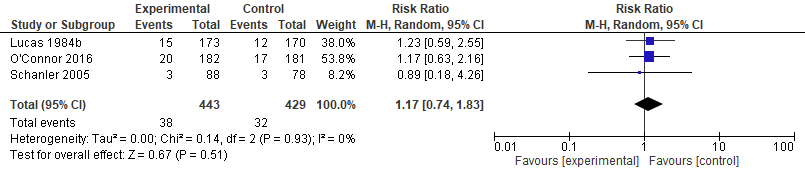
If we therefore meta-analyze those trials where babies seem to have received mother’s milk, and to have had a supplement of either donor milk, or artificial formula, and had their diet during the period of risk for NEC, we are left with just 2 fairly recent trials, and 1 much older trial, with the limitations noted above. This seems to confirm that artificial formula, as a supplement when there is insufficient mother’s milk, leads to a major increase in NEC compared to using donor human milk. Although the 95% confidence intervals are large, they do not include no difference, and all 3 of the trials are in the same direction with an I2 of 0. As you can see below there is no evidence of an impact on mortality, but the very small difference is in favour of donor milk.
There is no prima facie reason to think that the source of the proteins is the reason for the association between artificial formula and NEC. There are many differences between artificial formulas, pasteurized donor milk and preterm mother’s milk: the microbiome of the milk, the presence of Oligosaccharides (HMOs), the precise nature of those HMOs, the presence and concentration of intact human lactoferrin and immunoglobulins, the concentrations of insulin and leptin, and other components of milk are different between fresh maternal milk, pasteurized donor milk, and artificial formula.
So what is it about artificial formulas that leads to increased NEC? Is it related to disturbances in the intestinal microbiome?
A recent publication has reviewed the impacts of some food additives on the intestinal microbiome (Bancil AS, et al. Food Additive Emulsifiers and Their Impact on Gut Microbiome, Permeability, and Inflammation: Mechanistic Insights in Inflammatory Bowel Disease. J Crohns Colitis. 2021;15(6):1068-79). They review the extensive evidence, previously unknown to me, that a group of food additives, emulsifying agents, have been shown to have major impacts on the intestinal microbiome.
One of the emulsifiers that has an extensive record of altering the microbiome, and even being used to induce a model of ulcerative colitis in animals is Carrageenan, There is even a very recent review article describing all the adverse imapcts of Carrageenan, and how it causes colitis (Guo J, et al. How does carrageenan cause colitis? A review. Carbohydr Polym. 2023;302:120374). I was surprised, and disturbed, to see that Carrageenan is present in Similac special care 24 calorie milk. It is also present in Similac liquid fortifier, but not their powdered fortifier or the liquid fortifier with protein hydrolysate, nor indeed in Enfamil preterm formula, or Enfamil powdered or liquid fortifiers. They all also contain other ingredients, however, such as Soy Lecithin, and oils from various sources, used to provide DHA or ARA.
Any of the components of the artificial formulas that we give to preterm babies might have effects on their microbiome, or other effects on inflammation, or on the Toll-like receptors that are involved in the pathogenesis of NEC. Of note the preterm formula used in the 3 studies that I meta-analyzed above were not all the same, and indeed, the composition of the formulas may have changed between those publications and their current composition. The process of pasteurization induces changes in milk protein structure (including pasteurization of human milk, Sergius-Ronot M, et al. Impact of holder, high temperature short time and high hydrostatic pressure pasteurization methods on protein structure and aggregation in a human milk protein concentrate. Food Chem. 2022;374:131808.)
The take-home message: avoid artificial infant formulas during the period of risk for Necrotising Enterocolits. We don’t know why, but supplementing mother’s milk with artificial formula increases the risk compared to supplementing with donor human milk.






