
It seems that they do, perhaps a little bit!
There are now a confusing array of trials of supplementation of polyunsaturated fatty acids in preterm infants. They have compared various control diets to differing PUFA supplements. Many of them have used a long chain omega-3 fatty acid, Docosahexaenoic acid (DHA), and sometimes also Eciosapentaenoic acid (EPA), rarely ALA (alpha-linolenic acid). Some of the studies have also used arachidonic acid, an omega-6 PUFA, and they all try to make sure that the essential FAs, linolenic and linoleic acid are supplied in sufficient quantities.
This new publication (Gould JF, et al. Neonatal Docosahexaenoic Acid in Preterm Infants and Intelligence at 5 Years. N Engl J Med. 2022;387(17):1579-88) notes in the introduction that the current dietary recommendations for DHA intake of about 20 mg a day, are lower than the usual in utero accretion of DHA, most of which goes to the brain and is incorporated into neuronal membranes and is needed for synaptic function. There are a couple of previous tiny trials of DHA supplementation in term babies which suggest that Bayley Scores and problem solving might be improved with a bit more DHA among formula fed babies. The new publication is a follow up study to N3RO which was a multicentre RCT in about 1200 preterm babies <29 weeks gestation with the primary outcome being BPD. BPD was actually more frequent with the DHA supplementation, against all expectations. DHA in that study was started by oral supplementation within 3 days of starting oral feeding, which supplied an additional 60 mg/kg/d.
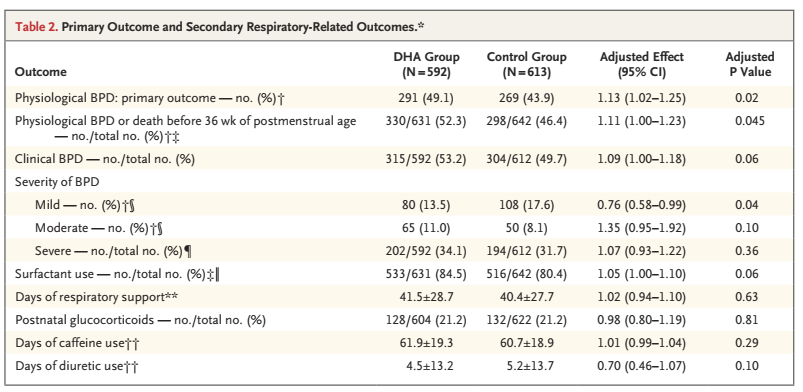
As you can see from the main outcome table from the original publication which is below, there was less mild BPD, but more moderate or severe BPD, and more BPD overall, with DHA supplementation.
The new publication is of a study in a subgroup of 480 Australian babies from the original trial with similar numbers and similar baseline characteristics in the 2 groups. The primary outcome for this study was the full scale IQ on the WPPSI at 5 years corrected age. Because of COVID a few evaluations were performed outside of the originally specified time window, and a few were unable to be tested.
The main results are below:
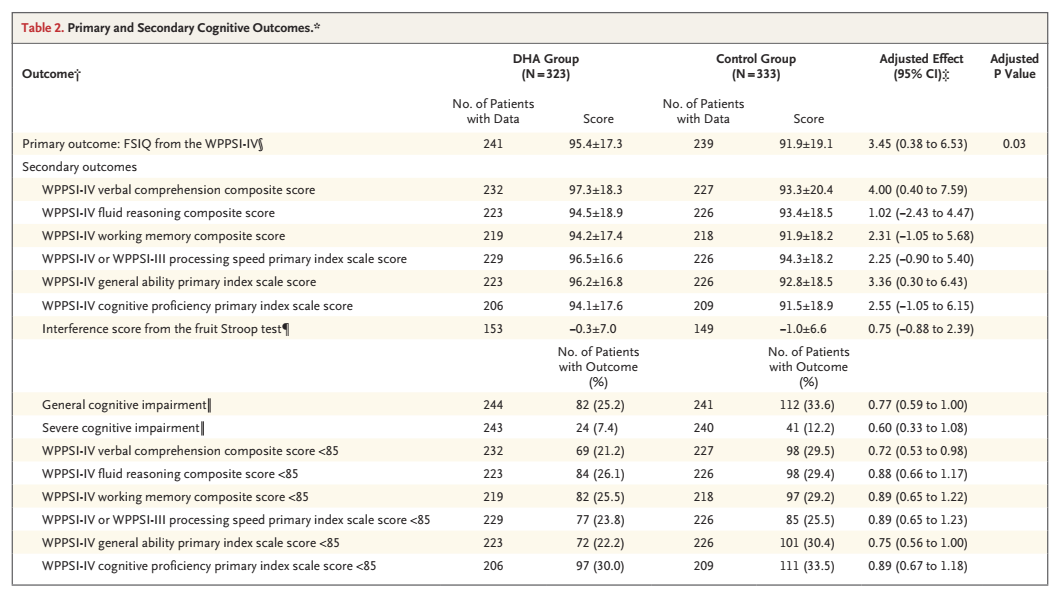
What they call “General Cognitive Impairment” is a WPSSI score less than 85 (it is a standardized score, so that is 1 SD below the mean) and “Severe Cognitive Impairment” is <70. In a sample with a normally distributed result, one would expect 16% to have General and 2.5% to have Severe Impairment.
One can see that the full scale scores are shifted up a few points in the DHA group, so that the mean is a little higher and fewer infants fall below those thresholds, and that the main difference is in verbal comprehension.
What should we do with these findings? First of all let’s try and put them in the context of other trials, the MOBYDick trial supplemented breast-feeding mothers of babies <29 weeks. The babies’ intake of DHA was probably less than in N3RO: supplementation increased the percentage of DHA in breast milk from 0.3% to just under 1% of total fatty acids, which remained at about 35 mg/mL, in other words a baby getting 100 mL/kg/d of breast milk from a supplemented mother would receive somewhere around 30 mg/kg/day of DHA compared to about 10 mg/kg/d in the controls. That study also showed an increase in BPD with supplementation, which was why they stopped the trial early, as the results of the N3RO trial appeared, and in combination with the increase in BPD on interim analysis of this trial they realized they were extremely unlikely to show a benefit. The 18 month follow up of that study (Guillot M, et al. Maternal High-Dose DHA Supplementation and Neurodevelopment at 18-22 Months of Preterm Children. Pediatrics. 2022;150(1)) showed no real differences between groups, with a slightly higher Bayley language composite score in the DHA supplemented group. On a subgroup analysis of that trial the scores were more improved in the more immature babies, but the statistical test for interaction suggests that might just be a random difference between the subgroups.
Another much smaller trial of DHA and AA supplementation in around 100 VLBW infants followed the babies to 6 months with the Ages and Stages questionnaire, which was improved on one subscale in the supplemented group, then to 2 years with Bayleys, and then to 8 years for IQ testing. The Bayley and IQ results were similar between the groups.
The DINO trial was an RCT, also from Australia, which enrolled infants of up to 33 weeks gestation, with both maternal supplementation or supplementation in formula milk, with the primary outcome being developmental outcomes. They showed no overall difference in Bayley scores at 18 months were similar between groups, with perhaps higher MDI scores by about 5 points in the supplemented girls.
This seems overall to suggest that there might be a slight benefit, overall, on developmental progress, of supplementation of the diet with DHA in very preterm infants, and at the least, there is unlikely to be a negative effect. It may be that there is a pro-inflammatory effect while receiving supplementation though, leading to an increase in oxygen needs at 36 weeks, and therefore the diagnosis of BPD. There is almost no longer term pulmonary follow up reported, however. The new report does mention that almost half of the babies in N3RO had a respiratory hospital admission before 5 years of age, with an average of just over 2 admissions; there was no real difference between the groups.
These studies point out again the major limitations of using “BPD” as the indicator of lung damage in the preterm infant. There is relatively poor correlation between BPD and longer term pulmonary outcomes which are of importance. It seems that supplementation with DHA may increase “BPD”, but does not increase long term pulmonary morbidity. It might make the babies a little bit smarter though.






