
I was searching through the lyrics of ELVIS songs for a quote that might be more apt for this new blog post than “It’s now or ever”, which I have used previously, when I realized that I am a loser, and I should spend more time with my kids!
The 2 year neurological and developmental outcomes of the ELVIS trial (Early vs Late Ventricular Intervention Study) have been published. Cizmeci MN, et al. Randomized Controlled Early versus Late Ventricular Intervention Study (ELVIS) in Posthemorrhagic Ventricular Dilatation: Outcome at 2 Years. The Journal of Pediatrics. 2020. Hopefully, you will remember (surely as a result of my previous ELVIS blog post) that this was a much-needed RCT comparing 2 strategies for intervening for post-haemorrhagic ventricular dilatation in preterm infants. You can imagine the importance of this study when you note that Linda de Vries, Floris Groenendaal, and Andy Whitelaw were all three involved in organizing and performing this trial. Post-haemorrhagic hydrocephalus (PHH, as I will call it from now on) has become less frequent over the years, as severe IVH has become less common, but it remains a major problem for a small number of babies.
In ELVIS, preterm infants under 35 weeks gestation who had an acute IVH with ventricular dilatation followed by progressive ventricular dilatation, were randomized to either of 2 approaches; in the early group:
treatment was started after the Ventricular Index had crossed p97 (97th percentile) but before crossing the p97+4 mm line, the Anterior Horn Width was >6 mm but <10 mm and/or the Thalamo-Occipital Distance was >25 mm. Intervention started with LPs (max 3), and if necessary, followed by insertion and taps from a Ventricular Reservoir, aiming for VI<p97 over the next 7–10 days.
In the late treatment group, the same sorts of interventions were performed, but they started when the ventricular index was greater than the 97th percentile + 4 mm, and the anterior horn width was over 10mm. This later threshold was based on old observational data, from Malcolm Levine I believe, that showed that once you passed this threshold progressive hydrocephalus was frequent. It had become a sort of default standard of care without any good data that it was the best indication for intervention.
In both groups, if a reservoir was inserted, it was tapped regularly
Ten mL/kg were removed once or twice a day, the volume adjusted according to cranial US. When taps from a reservoir were still needed 28 days after insertion to keep the ventricular index well below the p97+4 mm, one or two ‘challenges’ were performed with discontinuation of taps. Reservoir taps were resumed in case of expanding ventricles, clinical symptoms and/or excessive head growth. Taps were continued until infant’s weight reached 2000–2500 g and according to unit protocol, the protein had decreased to <1.5 g/L and erythrocytes <100/mm3, at which stage the infant became eligible for a VP shunt.
The primary outcome for the early phase of the study was whether or not you survived without needing a shunt.
As you might imagine, the early treatment group had many more LPs; and needed many more reservoirs, 40/64 compared to 27/62. They did not, however, need more VP shunts, in fact, slightly fewer shunts were needed with early treatment, 12 vs 14.
Of course what we really want to know is the long term outcomes, if they had been similar, then less intervention could be considered to always be a good thing, but if there was a difference between groups, then the increased need for intervention in the early group should be weighed against the outcomes. The 2 year follow up study analyzed outcomes from about 90% of survivors, so is a reliable indication of what outcomes to expect with these approaches.
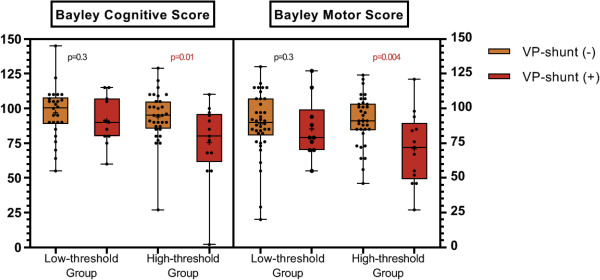
Bayley scores were better with earlier intervention, and there was less cerebral palsy; there was a relatively small sample size, and therefore the differences shown may have been random effects. This figure suggests that, among those needing shunts, the differences were greater than could be expected by random variation.
Adjusted analyses showed that early intervention seemed to be associated with a decreased risk of an adverse outcome after correcting for gestational age, the severity of intraventricular haemorrhage and cerebellar haemorrhage (adjusted odds ratio: 0.24, 95% confidence interval [CI], 0.07 to 0.87. In this situation, I think adverse outcome means death, or cerebral palsy, or a Bayley version 3 motor or cognitive composite score more than 2 SD below the mean.
It is interesting that in the early treatment group 94% of the cognitive scores were above -2SD with early treatment, and 87% with later treatment. The large majority of preterm infants with PHH who were enrolled in this trial, therefore, did NOT have cognitive delay! There is obviously a great deal of selection that goes on before an infant would be randomized in a trial such as this, but good outcomes of PHH are not rare! Motor scores were more severely affected than cognitive scores, but were also somewhat better in the early treatment group.
The clinical implications of this trial to me are that PHH should be treated according to the early intervention thresholds in ELVIS. The differences in outcomes are not enormous, but all favour earlier intervention. The only advantage of waiting until the later thresholds are crossed is that there are fewer lumbar punctures and fewer reservoirs, but no reduction in permanent shunts. I also think the study confirms that the Levine thresholds from many years ago were reasonable, and, I think should now be considered to be late treatment. Once the late treatment thresholds are reached intervention becomes urgent and should not be further delayed, unless there is an understanding with the parents that interventions will be limited. If we are aiming for the best possible long term outcomes, then the early treatment thresholds of ELVIS should be followed.
Otherwise, we may be accompanying ELVIS singing “Maybe its too late, I sometimes even hate myself…”







Why do LPs? Do they really decrease the proportion of babies who need a reservoir, or is it while waiting for surgery to happen?
Hi Annie, there is no much evidence that LP would help, see this review
J Neurosurg Pediatrics (Suppl) 14:8–23, 2014 ©AANS, 2014
Pediatric hydrocephalus: systematic literature review and evidence-based guidelines. Part 2: Management of posthemorrhagic hydrocephalus in premature infants
Catherine a. Mazzola, M.D.,1 asiM F. ChouDhri, M.D.,2,3 Kurtis i. auguste, M.D.,4 DaviD D. liMbriCK Jr., M.D., Ph.D.,5 Marta rogiDo, M.D.,6 laura MitChell, M.a.,7 anD ann Marie Flannery, M.D
This is what I thought, could not find an article to suppor this. Then isn’t it weird to make this part of an intervention in a large trial, when there is no evidence it should be part of such an intervention? Just worried with this study we will start doing LPs or be asked to do 3 LPs on all these babies before a shunt is considered.
The Elvis started 12 years ago and then LP were “state of the art” but there was no evidence for that. It shows that there is comunicación between ventricles and spinal space. Moreover there was not much experience on reservoirs placement, it was and is an intervention but it became simpler and requires less surgical time at the moment. I do not think that you should consider it in your clinical practice or for planning a trial
Thanks for the question Annie, and for the link to the guidelines development article Carlos, It is strange that that review did not include data from the largest trial ever performed for post-haemorrhagic hydrocephalus, slightly larger than ELVIS. I am speaking about the Ventriculomegaly Trial Group study, which randomized 157 babies with PHH to either get early “taps” (spinal or ventricular) or conventional treatment. The early group started repeated taps at 97th percentile plus 4 mm, and were shunted if they needed more than 4 weeks of taps. The conventional group were shunted if the head was growing too fast, or if the CSF pressure was high so some of them did get LPs, https://pubmed.ncbi.nlm.nih.gov/7512322/ follow up to 30 months of age was reported, and I think the primary outcome variable was severe impairment, but I am not sure how that was defined. Overall there were no big differences in outcomes between the groups, some small differences favoured the early intervention group, but they also had more meningitis. (7 infants compared to 4) In that study babies had repeated LPs for 4 weeks, and a median of 7 spinal or ventricular taps over the first 100 days of treatment, with the 90th %le being 37 taps!
I think the reason they included this phase in the 2 ELVIS groups was because of the difficulty in arranging immediate reservoir placement in many centres, and also perhaps because some babies have transient dilatation that does not need further surgical intervention. So in the early group, only 40 of the 64 randomized babies needed a reservoir, and in the late group it was 27/62. Their long term outcomes are better than in any of the previous studies of PHH, so I think we should be careful before dismissing an integral part of their treatment protocol. A maximum of 3 LPs while waiting up to 14 days to see if the ventricular dilatation progresses seems not an unreasonable approach, but if you are in a centre where transfer to a tertiary/quaternary NICU is required to get the baby shunted you should probably transfer them immediately you reach low treatment threshold criteria.
Hi Keith, sorry to insist but all this is your fault, we are now used to look for the best evidence and just then accept the use or not use of procedures in clinical practice. What I am pasting is coming from a sistematic review and the link is here:
Pediatric hydrocephalus: systematic literature review and evidence-based
guidelines. Part 2: Management of posthemorrhagic hydrocephalus in
premature infants
J Neurosurg Pediatrics (Suppl) 14:8–23, 2014
8 J Neurosurg: Pediatrics / Volume 14 / November 2014
©AANS, 2014
Routine Use of Serial Lumbar Puncture
Recommendation: The routine use of serial lumbar
puncture (LP) is not recommended to reduce the need for
shunt placement or to avoid the progression of hydrocephalus
in premature infants. Strength of Recommendation:
Level I, high degree of clinical certainty.
One Class I study was included, and it reported no
statistical differences in outcomes of preterm infants with
PHH treated with observation alone or infants treated
with daily LP (Table 2).4 Lumbar puncture is often used
early in the treatment of PHH, despite the fact that there
is no statistically significant reduction in the need for a
shunt or progression of PHH.4,54 In fact, LP neither predicts
nor prevents the need for a permanent VP shunt.36
A second study, a Class III study, also reported no difference
in adverse outcome regardless of whether infants
were untreated or treated with serial LP.15 Without aggressive
treatment of hydrocephalus and with persistent
ventricular dilation, outcome was poor.15 Additionally,
there was a single Class III study that concluded that repeated
LPs may cause or contribute to subsequent shunt
infection.6 Although LP may be useful for drawing off
CSF as an immediate treatment for elevated intracranial
pressure in infants with PHH, or for sampling CSF, we
do not recommend the routine use of LP to eliminate the
need for a VP shunt.15
I cannot find support for the use of LP as a way to arrests ventricular dilatation, besides LP requires handling of the baby, flexions, apnea, failure to find the spinal space, yieding of bood or not enough CSF volume. Besides there is a percentage of babys in whom VD arrests spontaneously.