
Retinopathy screening is undoubtedly painful for preterm babies, formal evaluation with PIPP scores routinely exceed 10 during screening, and may exceed 14, meaning moderate to severe pain. As a planned procedure there is always opportunity for pre-emptive analgesia prior to and during a screening exam, but what? Many of the interventions studied have limited efficacy.
A new systematic review has examined the efficacy of “pharmacologic” methods of pain control, and therefore, using their definition of “pharmacologic”, excluded breast milk, sucrose, swaddling; I know there has been some debate about whether sucrose should be considered “pharmacologic” or not, but that was the definition they used.
The review, which is unfortunately lacking in cute Forest plots to copy into this post, confirms that topical anaesthesia has limited effectiveness, there are 4 controlled trials that they found, with a mean PIPP score after local anaesthetic of between 10 and 15, reduced by an overall 1.6 points, which although not likely to be due to chance, is a very small reduction.
The other studies they reviewed all used topical anaesthesia in both groups, and examined other additional analgesia. They found 3 trials with acetaminophen (paracetamol to the Europeans) compared to control or placebo or sugar or milk. Overall, 2 of the trials showed a reduction in PIPP scores during the procedure, the 3rd reported PIPP scores after the procedure, which ere also reduced. The 3 trials used 15 or 20 mg/kg of acetaminophen given either 30 or 60 minutes prior to the procedure. As for opiates there were 2 trials of oral morphine which show relatively little effect, and one of intranasal fentanyl which appeared effective, when given in combination with sucrose and topical anaesthesia compared to that combination without fentanyl (Sindhur M, et al. Intranasal fentanyl for pain management during screening for retinopathy of prematurity in preterm infants: a randomized controlled trial. J Perinatol. 2020;40(6):881-7). That was a nice masked study with 50 babies per group, and has the advantage over acetaminophen that it works quickly, I don’t think it has become widespread, but why not?
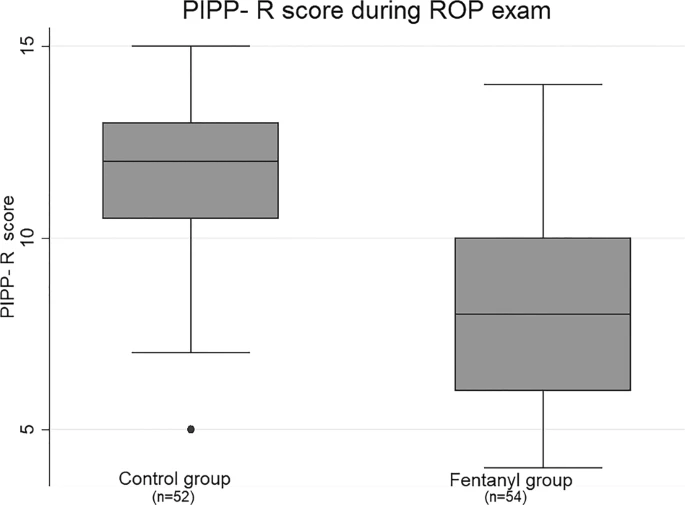
You can see from that figure, taken from the aforementioned publication, that intranasal fentanyl was rather effective. You can also see from the controls that despite topical anaesthesia, swaddling, and sucrose, retinopathy screening examinations still hurt.
Other interventions that have been tried include nitrous oxide, in a controlled trial by my friend Romain Mandel and our colleagues (Mandel R, et al. Nitrous oxide analgesia during retinopathy screening: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2012;97(2):F83-7) which didn’t have a benefit, Also breast milk, compared to sucrose, which showed that neither was better than placebo control for the acute pain response, but the breast milk babies apparently returned to baseline a bit faster than the sucrose, at least that is what the authors write (Şener Taplak A, Erdem E. A Comparison of Breast Milk and Sucrose in Reducing Neonatal Pain During Eye Exam for Retinopathy of Prematurity. Breastfeed Med. 2017;12(5):305-10), but I can’t see any data in the article to support that contention, the post procedure PIPP scores were lower in the 2 intervention groups compared to control, but there are no reported data about time to recovery.
What I make of all this is that topical anaesthetic is of limited efficacy, but I would still give it anyway, it seems 100% safe, and there is probably a small beneficial effect. Sucrose does very little if anything, but perhaps the babies return to baseline a little faster with either sucrose of breast milk, at the age when the babies are getting screened they are receiving much less sucrose for other procedures, so it will probably be safe to give; the use of breast milk as an alternative does not seem much more effective. Adding a pacifier/soother/dummy usually makes sucrose more effective, but for eye screening this has not been shown for sure, on the other had giving sucrose, with a soother/pacifier/dummy and swaddling does have some impact (O’Sullivan A, et al. Sweeten, soother and swaddle for retinopathy of prematurity screening: a randomised placebo controlled trial. Archives of Disease in Childhood – Fetal and Neonatal Edition. 2010;95(6):F419-F22).
I think that either acetaminophen or nasal fentanyl given before the procedure warrants either routine introduction or more study. I’d like to see confirmation of the efficacy and safety of routine intranasal fentanyl before introducing the practice to large numbers of stable preterm infants, but it does seem effective from that one study, and the dose of 2 microg/kg as a single administration in the nose appears from other data to be safe. The reduction of pain scores with acetaminophen is interesting but it isn’t apparently as effective as fentanyl, although a comparative trial would be nice.
My optimal protocol for the present would be, administration of 15 mg/kg of acetaminophen 30 to 60 minutes prior to the procedure, at the time of application of topical anaesthetic and mydriatic, swaddling of the baby and administration of sucrose 2 minutes prior to the procedure, a second dose of sucrose with a soother just prior to speculum insertion, then repeated sucrose if the procedure takes more than 2 minutes, and trying to avoid scleral depression if possible.






