
The first multicentre trial of bovine lactoferrin supplementation in preterm infants showed a dramatic reduction in late-onset sepsis of about 70%. I was very excited when I first saw Paolo Manzoni’s trial and rushed to set up a pilot in my NICU so that we could apply for funds to perform a confirmatory trial. The Lacuna trial which we published was not powered for sepsis outcomes, but for the feasibility of a subsequent masked multicentre RCT using our preparation, and ensuring that we could mask it easily. The proportion of babies with at least one infection was similar between our groups, but an exploratory analysis that I performed (and didn’t publish as it was unplanned and is therefore not scientifically reliable) suggested a reduction in infections per 100 patient days. That confirmed my desire to proceed with further trials.
The subsequent trials have generally shown only small differences in sepsis, with one or two exceptions from small trials. All the trials do show less sepsis with lactoferrin than control, but, in many of the trials, the difference was very small and may have been due to chance.
The most recent trial, LIFT Australia, is now published (Tarnow-Mordi WO, et al. The effect of lactoferrin supplementation on death or major morbidity in very low birthweight infants (LIFT): a multicentre, double-blind, randomised controlled trial. The Lancet Child & Adolescent Health. 2020;4(6):444-54). This was a multi-centre masked trial in 1500 infants of less than 1500g birthweight randomized during the first week of life. Unlike the original Manzoni trial, and my pilot, the dose was by body weight at 200 mg/kg/day. I gave everyone 100 mg/day, so except for a baby under 500g, this new trial gave more. The primary outcome of the trial was a composite of death, NEC (stage 2 or 3) Late-Onset Sepsis (LOS), retinopathy needing treatment, and brain injury. There was no difference in this outcome 21% vs 22%. The difference in LOS alone was very small 12% with lactoferrin and 14% in controls, it only included culture-positive sepsis.
The LIFT dose was higher than the previous, even larger, masked multi-centre trial from the UK in 2200 babies <32 weeks and ❤ days of age. (Griffiths J, et al. Enteral lactoferrin supplementation for very preterm infants: a randomised placebo-controlled trial. The Lancet. 2019;393(10170):423-33). This trial, known as ELFIN, gave 150 mg/kg. The primary outcome was LOS or “clinically suspected infection”, which was 29% in the lactoferrin group and 31% in controls. As frequent readers will know I am very sceptical about the occurrence of “culture-negative sepsis”, and their definition, which is given in detail in this publication, doesn’t make me any less sceptical. If we focus on confirmed LOS, the incidence was more similar to LIFT, 17% vs 17%, identical in the 2 groups.
One of the strengths of the LIFT trial is that in the publication they performed a PRISMA compliant systematic review of all the available evidence. That review suggested a decrease in Late-Onset Sepsis (LOS) with lactoferrin compared to control; as I mentioned before, all of the trials show fewer babies with LOS if they received Lactoferrin, but many of the studies had very small differences, including ELFIN, RR=0.94, and LIFT RR=0.83. However, as mentioned, this includes culture-negative sepsis in the ELFIN trial, but not in LIFT, or in Manzoni et al, or in Barrington et al (I didn’t check all the others, 2 are in Chinese and I can’t get hold of them anyway.)

The statistical tests of heterogeneity showed that the trials differed in this outcome. The I² from the random effects version of the meta-analysis is 58%, and the difference between trials is unlikely to be due to chance alone according to a chi-square analysis.
Why might this be? Of course, the difference between trials might just be a chance occurrence, but the statistical testing suggests it may be more than that. It is possible that the patients are different. One difference could be the breast milk intake of the babies. Maternal breast milk, unpasteurized, has higher concentrations of lactoferrin than pasteurized donor milk (human lactoferrin obviously), and there is almost no bovine lactoferrin in commercial formula. In the Lacuna trial, 90% of the babies received some maternal milk, and 60% had no formula at all, there was no donor milk at that time in our NICU. In ELFIN most of the babies received a mixture of formula and breast milk, secondary analysis suggests that there might be a differential impact of lactoferrin according to feed type, but it is not a clear difference between the groups., the statistical test for the interaction was not convincing. In LIFT there was a very high frequency of maternal breast milk use.
This may be one reason that we saw very little impact of lactoferrin supplementation on the intestinal microbiome of our babies, Grzywacz K, et al. Bovine Lactoferrin Supplementation Does Not Disrupt Microbiota Development in Preterm Infants Receiving Probiotics. J Pediatr Gastroenterol Nutr. 2020;71(2):216-22; in a side-study that we have just published among 70 of the 80 babies in our pilot, who were all receiving probiotics and mostly receiving breast milk, differences in microbiome development were minor between the probiotic group (P) and the probiotic with lactoferrin group (PL).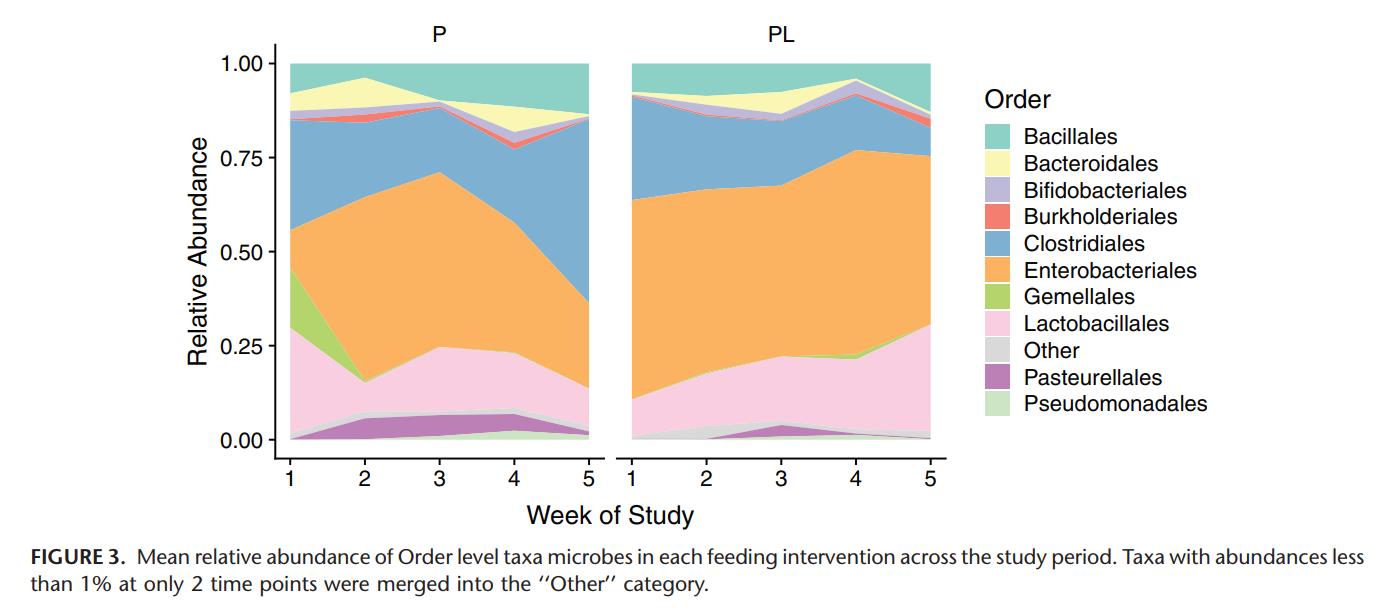
Breastfeeding rates were somewhat lower in the original Manzoni trial, and he has recently published a secondary analysis suggesting that lactoferrin was much more effective in babies receiving formula rather than breast milk. (Manzoni P, et al. Is Lactoferrin More Effective in Reducing Late-Onset Sepsis in Preterm Neonates Fed Formula Than in Those Receiving Mother’s Own Milk? Secondary Analyses of Two Multicenter Randomized Controlled Trials. Am J Perinatol. 2019;36(S 02):S120-S5) although after multivariate correction the data are less convincing.
I also wonder if we are all testing the same thing. Is all lactoferrin identical? A new publication from UC Davis shows that different sources of bovine lactoferrin have somewhat different properties, (Lönnerdal B, et al. Biological activities of commercial bovine lactoferrin sources. Biochem Cell Biol. 2020.) here, in what I believe is a first for the blog, is a Western blot!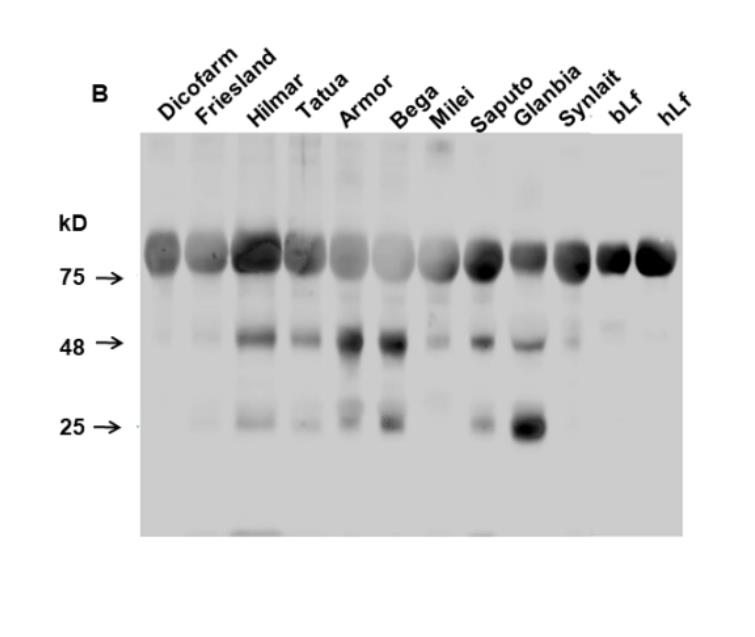
bLf is the lactoferrin as processed by the investigators themselves, showing a single band at 75 kD, similar to Dicofarm which was the Manzoni product, Tatua was the ELFIN product, showing in addition 2 other bands. LIFT used “Australia’s own” lactoferrin, which may not be identical to any of these, and LACUNA and LIFT Canada (currently underway) use a product supplied by AOR, which seems to have its origin in Australia.
hLf is human lactoferrin, which has a similar structure to bLf, but not identical.
The authors of this study also looked at bioactivity, using various assays, and did proteomic analysis showing some contamination with small concentrations of other bovine milk proteins.
In summary, it is apparent that the commercial Lfs we investigated have different degrees of purity and that the contaminating proteins also vary. There are considerable variations in the bioactivities among the Lf samples, but there is no discernible consistency such that one sample is high for all activities and another has overall low activities. The mechanisms behind NEC and sepsis are not known yet but likely involve mucosal integrity (cell differentiation), infection (EPEC) and immune response (cytokines), but since we do not know the relative involvement of each of these processes it is difficult to assess the reason(s) why some clinical trials have shown positive outcomes while others have not. Finally, there seems to be limited effects of pasteurization of Lf on its bioactivities.
I think this means that there is still potential that some preparation of bovine lactoferrin will have a significant impact on LOS in preterm infants. Also, lactoferrin has never been associated with adverse impacts. Because of the very important effect shown in the Manzoni trial it would be worthwhile to do other studies, to complete LIFT Canada, and any other trials underway, and then perhaps to do another trial with the Dicofarm product. I think we should focus on culture-positive sepsis and NEC, and hope that the original promise of lactoferrin will be found to lead to an effective way to reduce at least partially the high frequency of LOS in very preterm babies.







Hi Keith, congratulations for this very balanced and interesting overview. I learnt a lot from your updates. With my best wishes, Paolo M