
Not having looked after an adult for many years (although I did do a year of postgraduate training in adult internal medicine before switching to paediatrics; I thought I should practice on the old ones before subjecting children to my ministrations) I had never heard about renal denervation therapy for hypertension. The idea being that sympathetic renal stimulation is important in maintaining high blood pressure; so someone invented a catheter that you insert into the femoral artery, pass up into the renal artery and denervate the kidneys using radio-frequency pulses.
As a neonatologist, who tries to use physiology rather than fighting against it, this seems to me inherently unlikely to be effective, but smarter people than me thought it might work, and performed a couple of randomized trials with impressive, almost unbelievable results (30 mmHg reduction in systolic blood pressure), and even managed to get a case report in the PNEJM. The company making the catheter became very profitable and were sold for millions.
Unfortunately it probably doesn’t work.
An excellent editorial in the BMJ includes this figure
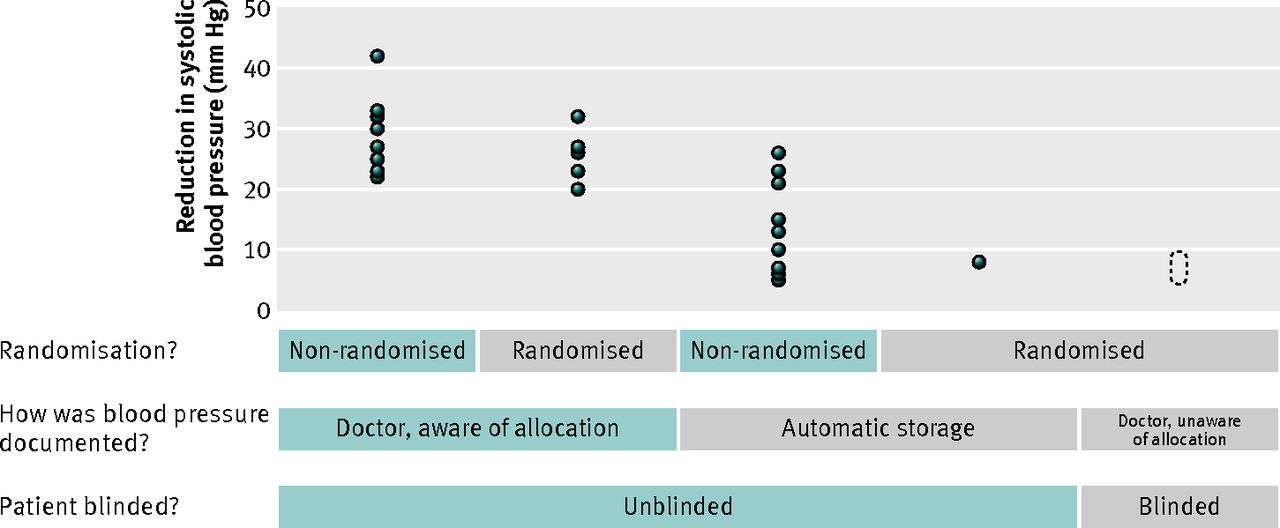
I like the subheading that precedes this figure ‘does my bias look big in this study?’ The figure shows the size of the apparent effectiveness of the intervention depending on the potential bias in the study design, each circle represents the systolic BP reduction from an individual trial. As you move from the unblinded studies where an unblinded investigator, who may have recently performed a highly invasive procedure on his patient, was responsible for recording the result, to masked randomized trials (with either automated BP measurement or a masked investigator taking the blood pressure), the effectiveness of the intervention disappears. The most recent, rigorous trial may show some residual minor benefit, but that is not clear. The trial has not even yet been published, but a press release from the company that bought the rights tot make the device states that they showed no benefit. A move they would only make if they didn’t find anything.
They did not show a substantial reduction in systolic blood pressure, even though the trial was designed to be able to find a 10 mmHg reduction.
The lessons are several.
1. Medical devices should be tested, with the same level of rigour as medications, before being licensed.
2. We should start with the most rigorous, least biased research designs, before huge financial resources are wasted, and patients potentially harmed. Which means that the first patient treated with a new intervention, be it a device, a procedure, or a drug, should be randomized and compared to best current practice.
3. In the long run it is cheaper to do the hard trials first, with randomization, blinding, objectively defined clinically important outcomes.
More from the BMJ editorial:
..ethics committees are responsible for protecting research participants’ “rights, safety, dignity, and wellbeing,” while balancing risks to participants against benefits to future patients. If the study is doomed to give the wrong answer, then no matter how small the risk, it is too large.
…interventional trials aimed at measuring efficacy without randomisation or blinding might be worse than useless. If so, they could be unethical by default.
Blinding isn’t always feasible, some trials are extremely difficult to blind: I remember one of my small studies which was comparing intubation using a muscle relaxant to without a muscle relaxant. It is easy to tell which babies are ‘paralyzed’, in fact you had to wait for the baby to be paralyzed before proceeding with the intubation. In such a case you must ensure that the data collected is completely objective, and that the enrollment is completed before the group assignment is revealed, that is, masking of the allocation.
We have to learn the lessons of trials like these, to avoid continually making the same mistakes. Unfortunately it seems the device is already licensed in Canada, clearly a huge mistake, we have to hope that doctors will just stop using it.






