Giving families a much greater role in the care of their infants is a really important advance and much of what Karel O’Brien and the team at Mount Sinai have done is what should be done in all our NICUs. O’Brien K, et al. Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: a multicentre, multinational, cluster-randomised controlled trial. The Lancet Child & Adolescent Health. 2018;2(4):245-54.
The idea behind family integrated care (FIC) is to give families much more room to participate in the care of their infants in the NICU, including participating in medical rounds, and becoming an essential part of the care team, including writing in the medical chart. It might even include adjustments of oxygen concentration and administration of some medications. It certainly includes eliminating institutional barriers to parental presence (such as sending parents away during hand-over or rounds; which used to happen in many places). I think we should be giving parents clear, overt, authority also to stop people touching their baby who haven’t washed their hands, or if they are the 2nd, 3rd or 4th member of the team (or consultant service) to examine the baby during a short time, or when the baby has just gone to sleep. Parents often don’t feel they have the right to intervene at such times, but recognizing their role as parents and putting them at the center of the care team could well help their baby.
If we change our approach to the place of parents in the NICU, what measurable outcomes should such an approach aim to achieve? Parents of hospitalised children, especially those who are critically ill, often feel disempowered, and have difficulty finding their place as parents. When your baby’s life starts in an NICU those difficulties are amplified, and may be associated with longer term issues in parenting and stress. So a trial of integrating families more into the care of their infants should probably examine outcomes such as parental feelings of empowerment, satisfaction and stress, parental resilience, how parents adjust, later on, to having their baby at home, whether they felt competent to be parents at home after discharge, whether they were less likely to be re-admitted during the first year of life (especially for more minor illnesses). Weight gain during the first few days after randomization, I suggest, is not something I would expect to be affected, nor would it interest me very much.
Empowering parents therefore is something I very much believe in, that being said this trial has a number of quite large problems, which make the conclusion, that family integrated care improves weight gain of infants born at 33 weeks gestation or less, between when the infants become stable enough to be enrolled (on CPAP or without respiratory support) and 21 days later, somewhat questionable.
This was a trial that was mostly a cluster randomized trial, but Mount Sinai hospital in Toronto, where the FIC approach was developed, was not randomized, they were a priori placed in the FIC group. As they are the largest inborn NICU in Canada, with, I think, about 1300 admissions a year, mostly of preterm babies, that immediately might create a bias in the results.
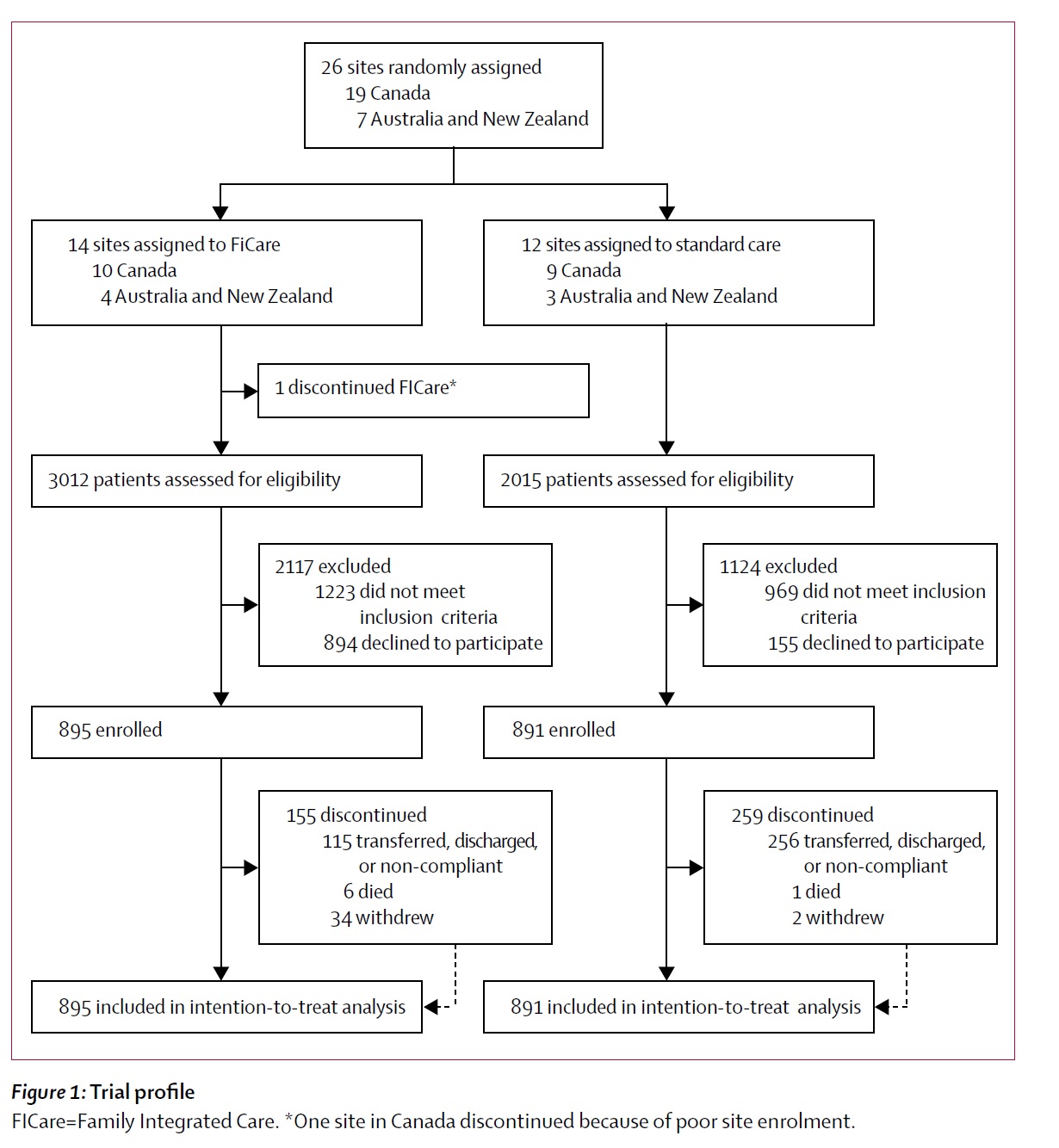
Parents enrolled in the FIC group were screened to ensure that they committed to “having a primary caregiver at the infant’s bedside for a minimum of 6 h per day (between 0700 h and 2000 h), 5 days a week, and to attend medical rounds and education sessions for at least 3 weeks”. Parents enrolled in the standard care hospitals didn’t have to give any such commitment. This immediately introduces another bias in this trial, which is critical to the results, the parents were therefore likely to be different between groups. A couple where one parent works full time, and that already has a young child at home, might not be able to give such a commitment, for example. You could easily imagine many other scenarios where that commitment would be difficult or impossible. This is probably one of the reasons why recruitment among eligible patients was very much lower in the FIC centers (30%) than the standard care centers (44%). If you look at the numbers differently, about half of the eligible patients in the FIC group (about 900 of about 1800) “declined” compared to only 15% of the controls (about 155 of about 1000). They had to approach 1.5 times as many patients in the FIC hospitals to enroll the same final number of infants. You can see those data here:
Several of the secondary outcomes might therefore be very different because of baseline differences between the groups; if a mother can be present for at least 6 hours per day, compared to a family that could not make that commitment, then breast feeding might well be different regardless of randomization. Breast-feeding outcomes at discharge were indeed different, or at least they were different between the modest proportion of babies for whom this outcome was available; which was only 396 of the FIC babies and 624 of the controls (of about 890 in each group). The breast feeding outcomes were only available for the infants who were not back-transported to step down level 2 care, which is something that occurred at a much higher frequency in the FIC centers, such centers might well have very different outcomes for breast-feeding, than infants discharged directly home from a tertiary NICU. I think therefore that the data on breast-feeding outcomes are quite unreliable, even though they are important, and might well be affected by an FIC approach, these data don’t really give us the answer about whether this approach improves breast-feeding at discharge.
One could also question the primary outcome, weight gain (or to be specific, change in weight z-score between enrolment and 21 days). Final weight z-score at discharge home, head circumference at discharge home, those are things which have an association with long term outcomes, but weight gain between about 32 weeks and about 35 weeks has a more questionable clinical significance. Weight gain is very closely associated with nutritional supply, so any difference in nutritional practices between the randomized institutions will have a big impact on this outcome. I can’t see in the published article a presentation of nutritional intakes or practices or of the intra-cluster correlation coefficients; maybe the centers randomized to standard care had nutritional standards which were less “aggressive” than the FIC NICUs. This is at least a possibility.
The results as presented show a change in body weight z-score of 1.58 in the FIC group and 1.45 in the standard care group; this I find impossible to understand, did body weight really cross multiple percentiles in both groups, to be about 1.5 standard deviations higher in each group, over 21 days?
I don’t think so, I think the primary outcome is not presented correctly, in fact the infants, on average, lost weight in comparison with Fenton’s growth trajectories, in both groups; but with a possible advantage in the FIC group.
Let me explain; when I look in detail at the results, the babies were on average 14oo grams at 32 weeks post-menstrual age when enrolled, and the mean z-score for their weight was -0.9 at that point (the same in both groups). If the groups had really both improved their z-scores by about 1.5 over 21 days, that would put them at about a weight z-score of +0.6, on average, at 35 weeks, which is about 2750 g, or an increase in 1350 grams on average over 21 days, a weight gain of, on average, 64 g per day. If that was true it would be remarkable, but, I suggest, close to impossible, and it is not what they report.
The article actually notes that the participants gained on average about 26 g/day, which would actually put them at just under 2 kg, on average, 21 days later; that is consistent with what the article reports as the percentage increase in body weight from enrolment to 21 days, of around 40% in both groups, a bit higher in the FIC group than the controls (42.6% vs 38.9%). What that means is that the z-score for the participants weight actually worsened from enrolment to 21 days. They went from an average of -0.9 to an average of about -1.3 for the z-score at 21 days, or a change in z-score of -0.3 (which is a long way from +1.5). Just to stay with the same z-score they would have had to gain about 31 g/day, so a small decrease in z-scores appears to be what they really showed, with what seems to be a lesser decrease in z-scores in the FIC group. I think therefore that the primary outcome is not presented correctly, although the results do seem to show a small weight gain advantage of the babies in the FIC centers, whether the z-score change is really different between groups is more questionable.
After messing around with these figures for a while I think that what they may have done is to recalculate the z-scores at 21 days after enrolment using the Fenton weight distributions as of the post-menstrual age of the date they were enrolled. So the controls for example, gained 24.8 grams a day between enrolment at an average of 32 weeks, and when they were re-weighed 21 days later. They were therefore at 35 weeks on average 1.962 kg body weight, which is equivalent to a weight z-score of 0.48 at 32 weeks. That is obviously an error if that is what was done, you can’t use weight z-scores calculated at 32 weeks for babies who were 35 weeks post-menstrual age!
The journal where this is published is not on my universities subscription list, and I had to wait a while to get the pdf via inter-library loans, which would be impossible if you weren’t part of a university; It also is not listed on Pubmed, and I can’t even get the supplementary appendix (to see what else is reported) without paying for it. Research funded by the Canadian Institutes of Health Research is supposed to be all publicly available, this currently isn’t. The CIHR rules are, unfortunately, not as stringent as the NIH, our rules are that within 12 months after publication, all research papers must be publicly available (either through the publisher’s website or an on-line repository). I think, as a side issue, that the CIHR should enforce immediate open-access of any research published using public funds (it would only add a few hundred dollars to studies costing tens, or hundreds of thousands of dollars or more). Both as a matter of good policy regarding the public’s capacity to read research that they funded, but also so that I can get a supplementary appendix!
In this study the parents in the FIC group (who started at slightly higher stress and anxiety scores than the standard care parents) had lower stress and anxiety scores at 21 days. Was that because of FIC, or because these parents were different to start with, or because of other factors in the NICUs that were in the FIC group? I wouldn’t be at all surprised if it was due to the FIC intervention…
What I am saying is this; integrating parents more in the care of their infants is a good thing. We should be ready to adjust our care models so that parents can do anything they want in the medical/nursing/respiratory care of their infants that is consistent with good safe practice. We should also avoid forcing parents to be “integrated” where they are not comfortable, not all parents want to be present during resuscitation, intubation, lumbar puncture and so on, and maybe some parents don’t want to write in the medical chart or present their infant during medical rounds. But, for those who do, there are an increasing number of publications (many of them based on the initiatives of Karel O’Brien and her colleagues from Mount Sinai Hospital in Toronto, such as this one from Glasgow in Scotland; Patel N, et al. Family Integrated Care: changing the culture in the neonatal unit. Archives of Disease in Childhood. 2018;103(5):415-9) which can give you interesting ideas about how to move forward,
Another recent publication shows that it is safe to have parents adjust the FiO2 of their babies (Martin-Pelegrina MD, et al. FiO2 control by parents of preterm infants admitted to a neonatal intensive care unit: A pilot study. Acta Paediatr. 2018) at least in a small pilot trial. After training the parents were allowed to adjust the FiO2, and the babies were less frequently hyperoxic, compared to controls.
This brings up another question I think, what do we need to know in order to change the culture in our NICU? I am not convinced, from these data, that FIC impacts weight gain; that does not stop me from wanting to make the NICU more welcoming, and more “integrating” of the parents of the babies I look after. It doesn’t stop me (and the rest of my team) from wanting to integrate many of the ideas of family integrated care into our practice at my hospital.
In fact, even if there was no difference between groups, and if, after eliminating Mount Sinai (the non-randomised center) from the results, and trying to correct for all the baseline differences between enrolled and non-enrolled parents, if after doing all that there was no impact on weight gain, or on other clinically important outcomes, then I would say that would be good evidence that we should be doing this. We should be allowing the integration of parents into the day to day medical, nursing, respiratory, physiotherapy, and feeding intervention care of their babies in the NICU; with training and supervision, at least as much as they want, and as much as they are capable of doing.
We also as a side note (and not related to this study) must not judge parents who feel unable, unprepared, or uncomfortable in performing these tasks. As mentioned above, I am not sure all parents want to do all of the things demanded by FIC; that doesn’t make them bad parents. If I think of how I was as an (unusual) NICU parent 14 years ago. I could not have spent 6 hours per day in the NICU, it was a pretty boring place most of the time! In the beautiful new unit where I now work, with the amazing private rooms with parents’ spaces etc, I would probably have spent a lot of my time on my laptop, writing blog posts, while my baby slept. I would appreciate the power to stop residents and others (even occasionally nurses) from touching my baby without adequate hand hygiene, but I don’t think I could have tolerated being there for 6 hours every day. I am not sure I would even have wanted to have the right to change the inspired oxygen concentration. Even though with my patients I fiddle with the FiO2 and the ventilator settings all the time (just ask my RT’s who get very irritated at times!) On the other hand, 12 hours a day looking after 30 babies and their families is just fine…