
The systematic review of the neonatal oxygen saturation targeting trials Askie LM, et al. Effects of targeting lower versus higher arterial oxygen saturations on death or disability in preterm infants. Cochrane database of systematic reviews (Online). 2017;4:Cd011190.
confirmed the increase in mortality with lower saturation targets (85 to 89%) compared to higher targets (91 to 95%) that was shown, in very preterm babies, by most of the individual trials, and showed very little heterogeneity between the trials. That review was limited to trials that enrolled patients at birth or soon after, and therefore excluded the first BOOST trial, and STOP-ROP. Those two trials enrolled children later in their hospital stay (for BOOST it was kids born before 30 weeks who still were on oxygen at 32 weeks, for STOP-ROP eligible babies had pre-threshold retinopathy and who needed oxygen to stay at or above 94%). They both randomly compared saturations in the low 90’s to saturations in the high 90’s
Despite the differences between the trials they both seemed to show somewhat worse pulmonary outcomes with higher saturations, including more babies on oxygen for longer, in STOP-ROP for example, at 3 months corrected age, well after the intervention had finished, there were 47% of the high saturation babies still on oxygen compared to 36% in the low saturation group. There were also twice as many babies still hospitalized at 3 months corrected (13% vs 7%), and more use of all the pulmonary medications reported. In the BOOST trial more babies went home on oxygen in the high saturation target group, but this could be predicted by trial design which maintained the target ranges for as long as the kids were in oxygen, so in the high saturation group it would be harder and take longer to be weaned off oxygen, by study design, They were also however, more likely to get steroids or diuretics, and more likely to be re-hospitalized during the first year of life and there were slightly more pulmonary deaths in the high saturation group. All of which suggests that targeting even higher saturations than the NeoPROM trials, and aiming for saturations above 94%, at least after the initial acute phase, might increase pulmonary oxygen toxicity enough to have an adverse clinical impact.
This new systematic review and meta-analysis (Chu DK, et al. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. The Lancet. 2018;391(10131):1693-705)
is one of a kind that I often criticise, studies of widely different patient populations are lumped together, so it doesn’t satisfy Barrington’s rule, that to be meta-analyzed patients should have been able to be eligible for each study. This review, however, searched for all studies of critically ill adults who were randomized to conservative or liberal oxygen strategies. It includes adults with a recent stroke, or septic shock or appendicitis, post-myocardial infarction or cardiac arrest. That makes me a bit sceptical about the applicability to all of those different groups, also the duration of the randomized intervention, and the actual oxygen concentrations administered where varied, although most of the conservative oxygen groups were on 21%. The authors found 25 randomized trials with a total of over 16000 patients, and overall, in the safety analysis, there was an increase in mortality. The benefit of doing a review like this is that you can get enough patients to find small changes in infrequent outcomes just by increasing the total numbers. In-hospital mortality was increased by 21%, which sound enormous, but in fact the increase was from about 3% to about 3.7%, 30 day mortality increased from 5.6% to 6.4%. Whether these differences really apply to all subgroups of patients is uncertain, but the review was not able to show any benefit of giving more oxygen.
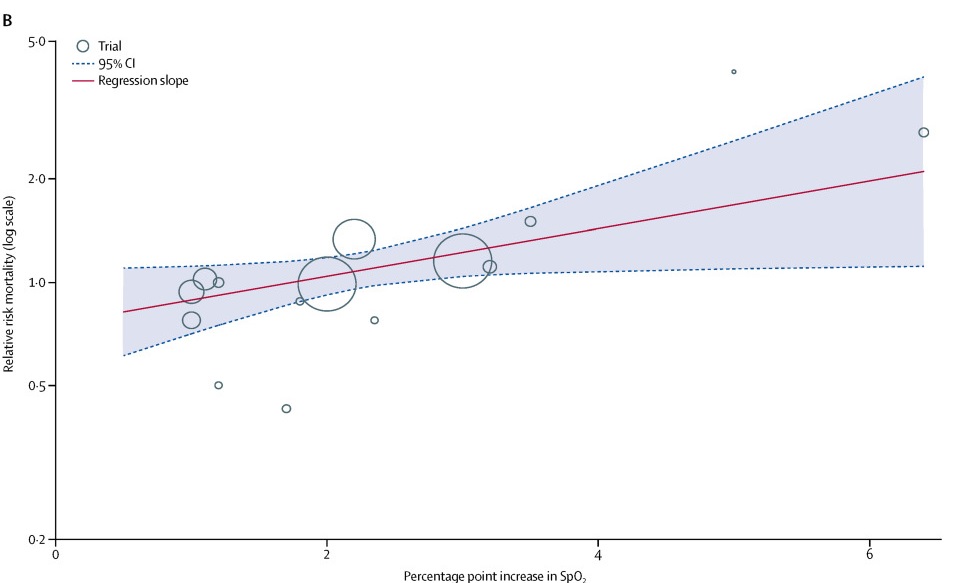
Another interesting finding from this review is that there seemed to be a dose effect, as saturations increased there was a greater effect on mortality, and the impact seemed to be significant above a saturation of about 94 to 96%.
Although we know in babies that mortality is lower with a target range of 91 to 95% than a range of 85 to 89%, we don’t know if there is a range that would have even lower mortality. In adults with varying serious illnesses, the upper limit of what you should aim for is probably around 95%, if your baseline saturation is above or close to 95% you should probably leave well alone and not give oxygen.
There are adverse effects of hyperoxia, even in full term babies and in mature experimental newborn animals, with an increase in pulmonary reactivity, and a reduction in the response to nitric oxide, as well as the generation of free radicals, and potential adverse effects on cardiac function (see this review). I think that much of what is discussed in the editorial accompanying the new systematic review could be transposed to our patients. Although the dangers of hyperoxia in very preterm babies have been appreciated for years, the potential dangers in later preterm and term babies are less well appreciated.






