
The upcoming issue of “Seminars in Perinatology” is about the controversies in caring for the babies <25 weeks gestation. Babies born at 24, 23, 22 or even now 21 weeks gestation are so physiologically immature that we can’t just assume that something that works at 28 weeks will also be beneficial for that sub-group. My contribution to the collection of articles (Barrington KJ. The most immature infants: Is evidence-based practice possible? Semin Perinatol. 2021:151543) was an attempt to find data about the most immature babies from recent large RCTs, the kind of evidence base that is reliable for determining treatment options. I searched large multi-centre RCTs from the last 5 years, and found 30 trials enrolling a total of over 25,000 very preterm infants. Many trials excluded the most immature babies, either formally by setting a lower limit for gestational age, or by being performed in countries (France and Holland) where active treatment at 22 and 23 weeks is absent or rare, and even at 24 weeks is (or was) quite limited. I could finally find only 3 babies of 22 weeks whose data were presented in those studies, and very few who were clearly of 23 weeks gestation. There were three trials that reported results by GA strata that included a stratum <25 weeks, and those trials, in total, included 711 babies.
Our entire evidence-base for therapies in the most immature babies is thus extremely limited, and most things that we have questions about are uncertain for those babies. That uncertainty can be seen in other articles of the series, such as this one (Sindelar R, et al. Respiratory management for extremely premature infants born at 22 to 23 weeks of gestation in proactive centers in Sweden, Japan, and USA. Semin Perinatol. 2021:151540) in which Richard Sindelar and his co-authors describe how different centers use assisted ventilation for the profoundly immature. In Uppsala, Sweden they start the babies on “conventional” ventilation with volume guarantee, and are able to maintain the majority of their babies like this, in Iowa, USA they start the infants on high-frequency jet ventilation and extubate at 850 grams minimum, in Kanagawa, Japan they start on conventional ventilation but change to high-frequency oscillation early if cardiac function is good. The authors describe a few points in common in their approaches, and one that is not mentioned. They have in common the use of 2.0 mm ETT for the 22 weeks infants, a focus on preventing over-distension, especially with the oversight of experienced clinicians, minimal handling, not trying to extubate too early, and giving surfactant very early. What they don’t mention is probably the most important factor; a belief that good survival is possible, that good long term outcomes are usual, and that it really is worth it.
To follow on from my previous post, there is also an article from Thuy Mai-Luu who runs our follow-up program at Sainte Justine, and Rebecca Pearce, an ex-NICU parent. They discuss how to improve neonatal follow-up to make it more relevant to parents, they include the following table:
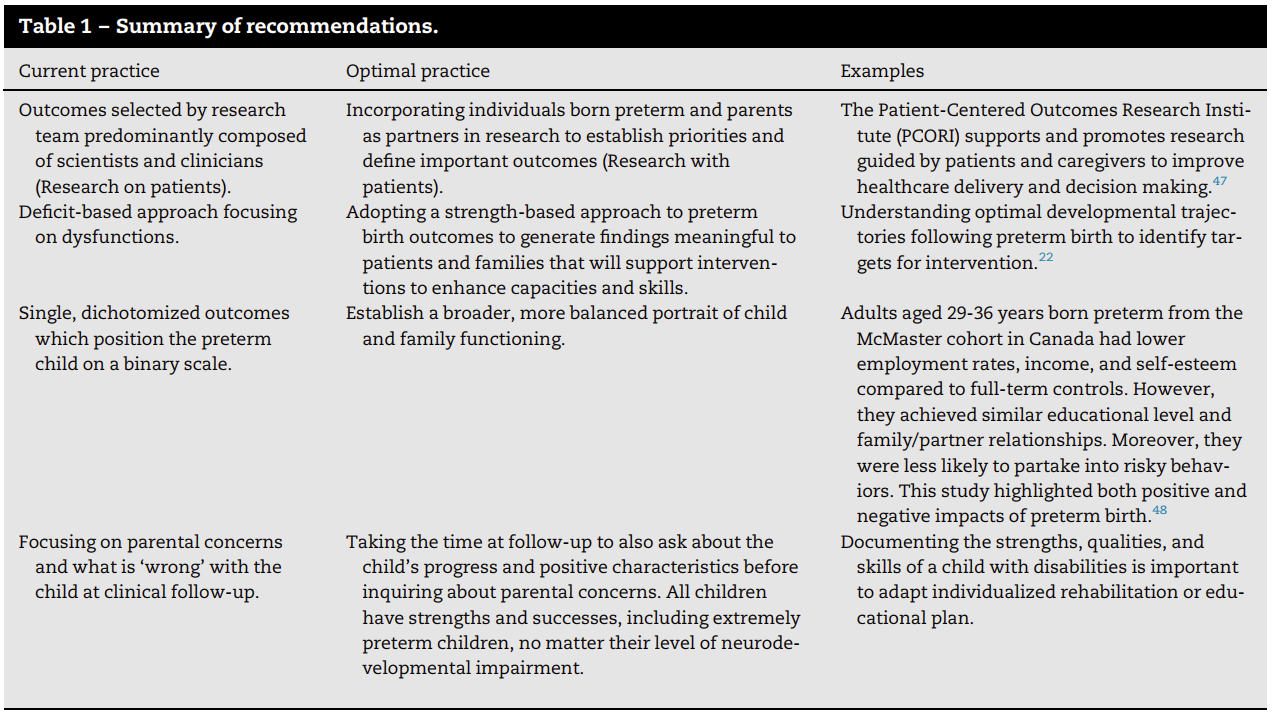
The focus on examining the strengths, rather than just the weaknesses, of former preterm infants, and avoiding simplistic dichotomised outcomes in favour of a broader, more balanced portrait of functions, are approaches that I absolutely agree with.
There are several other articles in this issue that should have a major impact on how we practice, including a pro-active integrated approach to the mother with her fetus, the nursing approach to these babies and their parents, and many others, all of which I would recommend. Given the possibility of more than 50% survival at 22 weeks gestation, shown by several groups, it is no longer ethically justifiable to universally deny intervention to such infants. But as we plan our intervention strategies for such babies we should all be listening to the experts and learn from how they have been able to get such good results.







Thank you very much for this commentary. I do agree that as we continue down the path of offering chance for life to the most immature babies, we need to really use our knowledge of fetal physiology to guide our approach. We can’t simply rely on studies of babies 25 weeks and older.
I think it is also very important to really partner with parents and as much as I agree that we need to focus on the positive outcomes of these babies, we also need to be ready to listen to parents who after soul searching, decide that they don’t want to continue active care and ask to redirect care to comfort.
I think our community is more ready to withhold care in the delivery room per parents request but when it comes to withdrawal of care in NICU per parents request we are looking for some ominous signs -grade 4 IVH, respiratory failure, renal failure etc but are unwilling to support the parents that make this very difficult and painful decision to just let their very premature baby die peacefully.
I believe that if we are to push the limits lower and lower we have to partner with parents and support them in their decision making no matter how uncomfortable it may make us,
In our NICU, and in most, I think, the majority of deaths follow a decision to limit or to redirect care. Verhagen AAE, et al. Categorizing Neonatal Deaths: A Cross-Cultural Study in the United States, Canada, and The Netherlands. The Journal of Pediatrics. 2010;156(1):33-7. Our centre was the Canadian centre in this study.
I think, as Bill Meadow used to say, that a “trial of care” is often the best approach for the most immature babies, which implies, of course, that we will withdraw active care later after starting ICU if we and the parents agree that it isn’t going well.