
The PREMILOC trial was a multi-center RCT of hydrocortisone, 0.5mg/kg twice per
day for 7 days followed by 0.5 mg/kg per day for 3 days, given starting within 24 hours of age to infants of 24 to less than 28 weeks gestation.
Neurological and developmental follow-up has just been published (Baud O, et al. Association between early low-dose hydrocortisone therapy in extremely preterm neonates and neurodevelopmental outcomes at 2 years of age. JAMA. 2017;317(13):1329-37.)
There were 523 infants initially enrolled and 406 who survived to 2 years of age, 93% of those were seen at between 21 and 23 months corrected age, for examination and evaluation with standardized instruments.
You probably remember that the primary outcome of the trial was survival without BPD, which was somewhat reduced by the intervention (51% compared to 60% in controls). This was as a result of fewer deaths (18% compared to 23%) and less BPD (22% compared to 26%) neither of which component of the primary outcome was individually significant. In this follow-up study the authors not that after the 36 week end of the main data collection there were a further 8 deaths, 7 in the control group and 1 in the hydrocortisone group, 5 of which were from severe BPD (4 vs 1). (These deaths were also reported as the deaths before discharge in the initial publication, but I don’t think the causes were noted).
All of the babies followed had a standardized neurologic evaluation, but unfortunately only 80% of them had the revised Brunet-Lézine evaluation of developmental progress, which gives a developmental quotient, standardized, as usual, with a population mean of 100 and SD of 15.
Basically there were no differences between the groups on neurological signs of impairment, or developmental scores. For example there were 6% of the hydrocortisone and 5% of the control group who developed cerebral palsy. Mean Global Development score was 91.7 in the hydrocortisone group and 91.4 in the control group.
I guess one could say that if there is less BPD and no increase in neuro or developmental adverse effects, we should think of using this as routine therapy?
But the group also report clinically important respiratory outcomes up to 2 years of age :
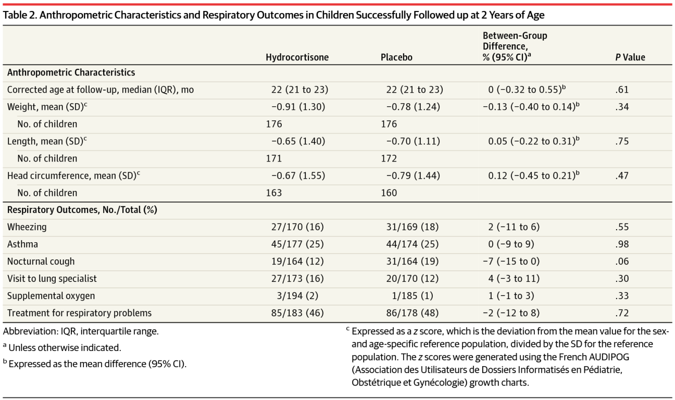
You can see from their table 2 that there is no sign of better respiratory health (or incidentally any effect on growth outcomes) among the survivors, with some of the minor differences being in one direction, some in the other direction.
Which calls into question again the use of oxygen at 36 weeks, as an outcome for RCTs even when combined with an oxygen reduction test, as in this trial. If kids are more likely to be out of oxygen at 36 weeks, but no more likely to go home on oxygen (14 babies in each group) and not more likely to have respiratory problems in follow-up, then the significance of getting extubated earlier, or needing oxygen for fewer days is questionable, at least the significance to families.
I think those outcomes are indeed benefits to families, its much better to see your baby with CPAP or non-invasive ventilation than intubated, but if there is on clear long-term benefit then we should be pretty certain that there is no harm before instituting this as routine therapy.
Currently, is there any other evidence of harm from this approach?
In the initial data from this trial, late onset sepsis was higher (31% vs 25% had at least one episode), NEC was higher (7% vs 5%) GI perforation was higher (5% vs 4%) use of insulin for hyperglycemia was higher (38% vs 34%) and severe RoP was higher (2% vs 1%) all of which could be due to chance effects, but the study was not powered to detect such small, but potentially important, differences; indeed in one subgroup, the most immature infants, the impact of steroids on late onset sepsis was, indeed quite different, 40% vs 23%, and their analysis showed this was unlikely due to chance. Its interesting in the on-line supplementary appendix that the major difference in late onset sepsis arose after the end of the treatment period.
It is also interesting that this dose of hydrocortisone had no evident impact on blood pressures, nor on the use of dopamine.
I think that all of these worrying differences between the groups, favoring control, with no evidence of long-term benefit, and the only evidence of short-term benefit being shorter intubation and shorter duration of oxygen therapy, that we should not introduce this regime as a routine in our patients.
There is a minor difference in survival with the hydrocortisone treatment though, with 19% mortality before discharge (and before 2 years) compared to 25% in the control group. I calculate the 95% confidence intervals of this 6% difference as being between 13% fewer deaths and 1% more deaths, using early low dose hydrocortisone in similar babies.
Unfortunately, I think I have to say that this therefore warrants further study. A larger trial with enough power to detect a 5% difference in mortality, perhaps in a region where the survival at 24 and 25 weeks is above 65% (as in this French multi-center trial; compared to for example 78% in the CNN database from 2015) should be performed.
I think a future trial should not use this as a definition of bronchopulmonary dysplasia, other definitions have been suggested, such as this recent publication from the CNN (Isayama T, et al. Revisiting the Definition of Bronchopulmonary Dysplasia: Effect of Changing Panoply of Respiratory Support for Preterm Neonates. JAMA Pediatr. 2017;171(3):271-9.) In this study the best discrimination between those who had serious respiratory morbidity after discharge (when seen at 18 month follow up) from data collected during the neonatal period, was the need for oxygen or respiratory support (anything that gave positive pressure including high-flow cannulae at more than 1.5 litres per minute) at 40 weeks post-menstrual age.
Serious respiratory morbidity was defined as either (1) 3 or more rehospitalizations after NICU discharge owing to respiratory problems (infectious or noninfectious); (2) having a tracheostomy; (3) using respiratory monitoring or support devices at home such as an apnea monitor or pulse oximeter; and (4) being on home oxygen or continuous positive airway pressure at the time of assessment between 18 and 21 months corrected age.
Just as important, a recognition that lung injury in the newborn is a continuous spectrum, and that artificially dividing that into 2 categories, with and without lung injury is an artificial distinction designed to aid research design, not to help babies, or their families. A description of long term respiratory morbidity between groups is essential, rather than a label based on an intermediate outcoem. Mortality, in contrast, is truly a dichotomous outcome, and if it can possibly be improved by low dose early hydrocortisone, than we should pursue that possibility with more studies.






