
We all need some iodine in order to make thyroid hormones (iodine doesn’t actually do anything else for us as far as I know), but do preterm babies get enough? They may need more than older children as they have very small stores, but it also is easy to make them toxic. One of my colleagues and friends, Tony Ryan, I remember as a fellow showed that using iodine containing liquids to lavage the peritoneum during surgery for perforated bowel caused hypothyroxinemia.
I also remember starting a research project to prove whether echocardiographic signs of cardiac output were reliable, performing a dye-dilution cardiac output study on a full term baby, to compare with ultrasound parameters. The dye I used, indocyanine green, contained a lot of iodine, so I had previously decided to do thyroid function studies to make sure that there was no impact. The very first patient had seriously deranged thyroid function after the first study, so the research stopped dead in its tracks (the baby did fine).
Preterm babies receive very little iodine during intravenous feeding, and it has been thought that many preterm babies are deficient, contributing to low thyroxine levels which are statistically associated with poorer developmental outcomes.
So if preterm babies really are frequently iodine deficient, then giving more should improve thyroxine production, which might possibly improve developmental outcomes (if the link between low T4 and slower development is causal). In contrast if too much is given, then transient thyroid suppression can occur. So we need a large, well designed, adequately powered, pragmatic clinical trial to answer the questions.
And here it is.
1273 babies in the UK who were all less than 31 weeks gestation were randomised in the first 2 days of life to receive sodium iodide, or placebo. They received 30 microg/kg per day, either intravenously or enterally until 34 weeks post-menstrual age. The primary outcome variable was the Bayley III scores at 2 years corrected age.
There was absolutely no detectable effect of supplementation with sodium iodide on outcomes. There was little effect on T4 or TSH either, with a small elevation of TSH levels in the iodide supplemented group in some groups at some postnatal ages, but no impact on T4.
288 infants were defined as being hypothyroid, with T4 less than the 10th %le, which looks odd at first how can 20% be below the 10th percentile? Infants were called hypothyroid if they were below that cutoff on any one of 3 occasions, day 7, 14 or 28, which explains this. On subgroup analysis, among hypothyroid infants, there were some signs of a minor benefit:
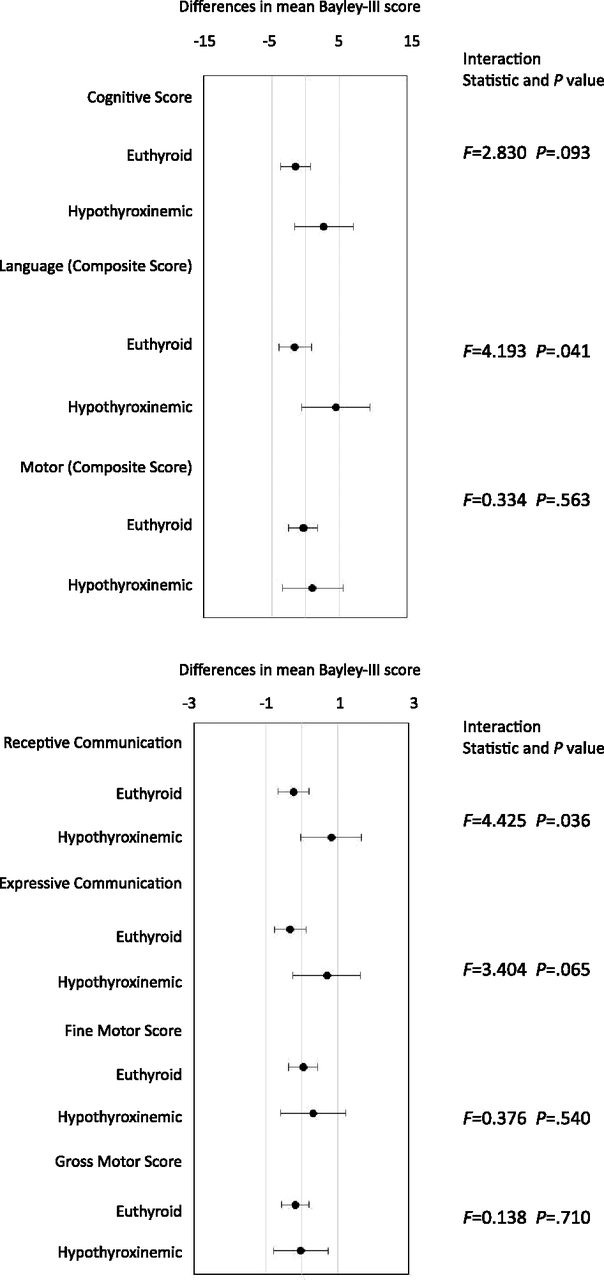
These figures show the mean differences between iodide supplemented and control infants for the various domains of the Bayley Scales. The hypothyroid babies who received iodide have slightly higher scores than controls on the cognitive and language scales. The euthyroid babies in contrast had very slightly lower scores.
The implications are, I think, that, overall, our babies are already receiving as much iodine as they need for their thyroid function, and for their development. There may be a small subgroup who are hypothyroid and might benefit from a supplement, but it is difficult to identify them, and not certain that there is a clinically significant impact.






