
In a recent post I promoted a new Barrington rule for meta-analysis (it probably already existed somewhere but I am claiming priority anyway, it’s a “post-truth” kind of thing). The rule was that in a systematic review you shouldn’t pool data from 2 (or more) studies if it was impossible to be eligible for all the studies, in other words, if there is no overlap in the eligibility criteria. For example in the systematic review of inhaled NO in the preterm, there were studies of early rescue use for critically ill babies, and studies of much later use in relatively stable babies. Combining all those studies makes little sense as it doesn’t answer any clinically useful question. If you want to know about the proven effects of early use of inhaled NO for a 12 hour old baby who is needing 100% oxygen, then adding into the analysis studies of babies who were studied because they were on CPAP at 2 weeks of age is really unhelpful, and will only muddy the waters.
Which is why I really don’t understand the rationale for mixing together several of the studies in this new meta-analysis and systematic review
The authors have included trials that studied :
(1) preterm infants of gestational age 22 0/7 to 36 6/7 weeks considered to be at risk for BPD, including both ventilated and nonventilated infants and (2) an RCT comparing any Inhaled Corticosteroid versus control (placebo or no treatment) at any dose and any duration of treatment and administered either by a metered-dose inhaler or by nebulization.
Which means they included studies with very early enrollment studying prophylaxis, other studies enrolling at 2 weeks of age of babies still intubated and with early BPD changes, and even one study that enrolled babies at 14 weeks of age who had already failed extubation and were needing more than 40% oxygen. I can’t imagine a clinical situation in which it would be useful to know the effects of inhaled steroids from all of those studies pooled data.
Most of the 16 included studies were tiny, with only 2 enrolling more than 100 babies, and most being around 30. Meta-analyzing multiple small studies risks inflating effect sizes. That isn’t the SR authors fault, but it is a problem with many neonatal systematic reviews.
The major primary outcome of the meta-analysis of Death or BPD at 36 weeks GA was based on 6 studies which are mostly somewhat similar to each other, and enrolled babies in the first 3 days of age (either on day one or on day 3) except for the study by Cole, which entered babies between 3 and 14 days of age. Bassler’s trial was a trial of prophylaxis in any baby needing assisted ventilation, whereas the others mostly needed some severity of illness criterion.
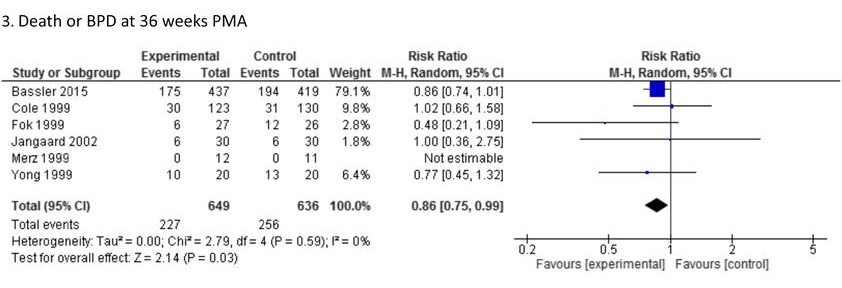
As I posted at the time that Bassler’s study was published that outcome is quite problematic, lung injury is a continuum, and forcing it into a dichotomous outcome for simplicity of reporting or analysis is rather unhelpful. Oxygen stopped at 35 weeks and 5 days, = no BPD, oxygen stopped 2 days later = BPD, even though the baby out of oxygen just before 36 weeks may have more signs of tachypnoea, retractions etc. Our recent publication (Janvier A, et al. Measuring and communicating meaningful outcomes in neonatology: A family perspective. Semin Perinatol. 2016) discusses this in some detail, and noted:
Many pulmonary outcomes having a negative impact on neonates and their families, such as rehospitalisation, needing oxygen therapy at home, and visits to the emergency department, are not systematically reported. A description of the impacts of the lung injury beyond a dichotomous BPD outcome would be much more useful, both to parents and to the health care professionals who care for them.
Although it is possible that very early inhaled steroids really do reduce oxygen requirements at 36 weeks, I am not sure this systematic review meta-analysis helps us know.
If you have a very preterm baby who is on respiratory support on the first day of life, and you want to know whether you should give inhaled steroids to reduce lung injury then the results of the studies in that Forest plot above from Yong, Fok and Bassler are relevant. In contrast, if the baby is not extubated by day 3 then the other studies are relevant, (Cole, Jangaard, and Merx). And even with all the data from both groups of studies that have non-overlapping eligibility criteria, the 95% confidence intervals are very close to 1.0.
So this isn’t really conclusive data, even about that outcome, death or BPD (of note there is no hint of an effect on death, the part of that outcome which is affected is the need for oxygen at 36 weeks), and as I said, I really don’t think it’s that important an outcome, unless, in this group, the diagnosis of BPD reflects worse pulmonary disease-related quality of life. What is now called moderate or worse BPD (i.e. oxygen for at least 28 days and still needing oxygen at 6 weeks) is associated with slightly worse long-term pulmonary function during the first year than mild BPD or no BPD, the differences are, however, not enormous. But just because a particular intervention decreases O2 requirements at 36 weeks doesn’t necessarily mean that those other clinically important outcomes (hospital re-admission, chronic pulmonary medication use etc) will be affected also. What I mean is, that steroids may reduce inflammation and have multiple effects on the lung, some of which might be negative, but unless they improve long-term lung function the baby hasn’t necessarily benefited.
I hope this Systematic review doesn’t lead to widespread use of a therapy for which the data are currently very limited, the excellent NEUROSIS trial will hopefully provide data about longer term pulmonary outcomes of their babies, to know if there is a benefit that will have an impact on the babies’ lives, and their families.






