
Our weeks are made of 7 days. An entirely arbitrary unit of measurement, based on an idea that 7 is magical, so there are 7 continents, 7 seas, 7 days of the week. Or maybe because you can easily divide a lunar month by 4, in fact it isn’t totally clear why there are 7 days in a week. It is hidden in the mists of time, the majority of human cultures use the 7 day week. But what if it had been 5? What if the Aztec system of 20 day periods, divided into 5 day weeks, had taken over?
2 day weekends and 3 days of work sounds like fun. Of course the duration of a pregnancy in Aztec land would be 56 five-day weeks, and then what we now refer to as 25 weeks gestation would become 35 five-day Aztec weeks. Neonatal survival becomes less and less likely as we descend to 34 Aztec weeks, or 33, and so on. But imagine if you were in an Aztec country,and the local paediatric society had recommended that “33 weekers” were not viable, because survival is too low, or impairment is to high (actually they don’t ever explicitly say why 33 weekers should not get active care) . Imagine if you were denied active intervention because you were only at “33 weeks” and 4 days, and told to go away until you hit 34 weeks. You could maybe just fly to Canada to find that you were suddenly viable, as you were 24 weeks and 1 day in 7-day weeks.
You could be forgiven for being a bit angry about your local paediatric society’s guidelines, especially when you realize that your ultrasound performed at 16 Aztec weeks was only accurate to within about one 5-day week, 95% of the time.
I’ve been thinking about this recently. Especially after the publication of the NICHD network data on active treatment, and how it changes by weeks of gestational age. One of the graphs from that publication shows that active intervention at 22 and 23 weeks stays relatively unchanged as a proportion of deliveries until just before the end of the week.
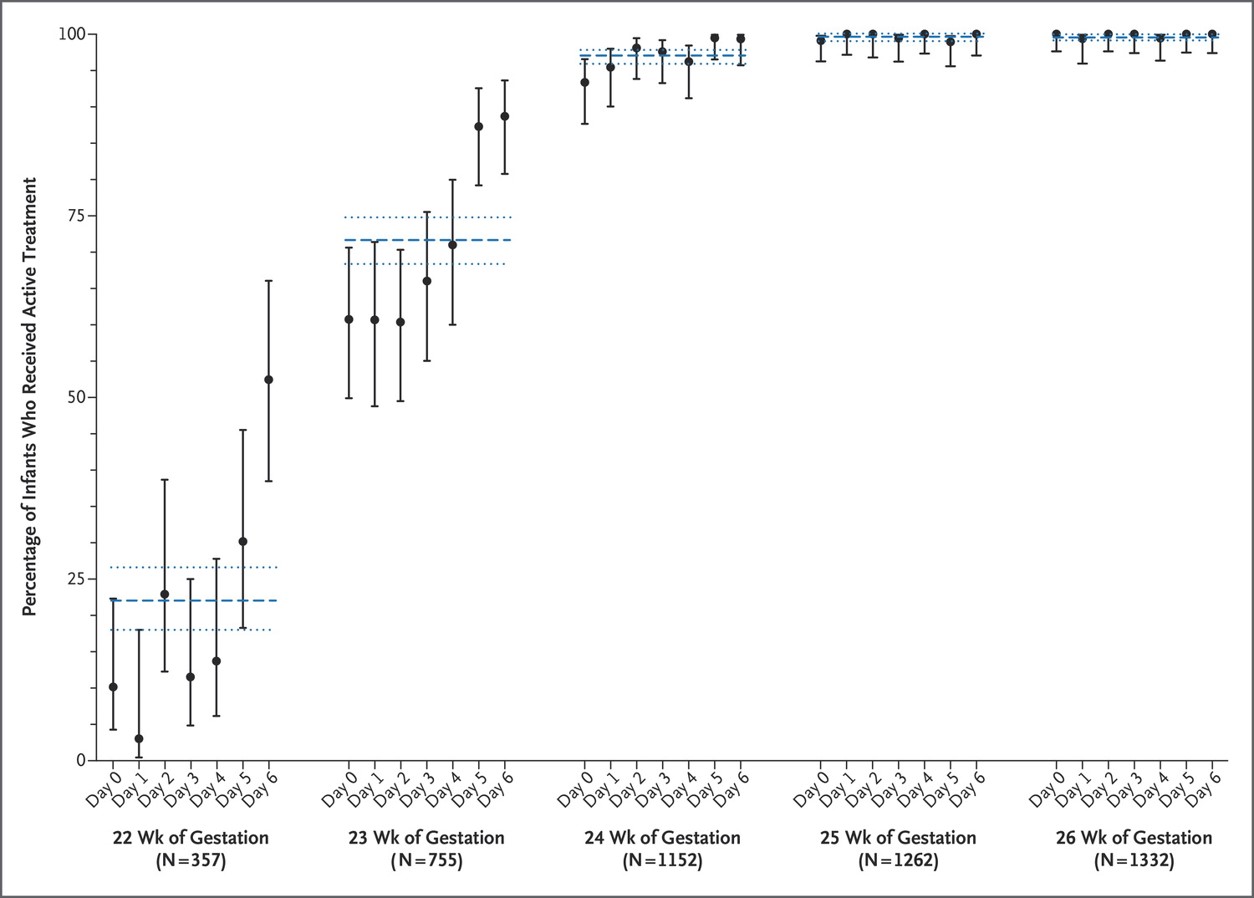
Which is odd, but I think easy to understand. We have become used to thinking of babies in terms of whole numbers of weeks of gestation. So a baby of 23 0/7 is thought of as being the same as 23 5/7. But once the baby is within 48 hours of the next big number, at which point they may have had steroids because of crazy hospital policies, based on 7 being the magical number, our attitudes start to change. I would be fascinated to know when the mothers got their steroids, and if that is really the cause of the jump up in intervention rates.
I would also be fascinated to see what the pattern would be in Aztec land.
One other thing that I think this shows, is that shared decision-making is currently a sham. Surely if mothers were adequately informed, and truly participated in the decisions, rather than having them imposed by physicians or by hospital practice, then there would be a progressive gradual increase in intervention as gestational age advanced. Mothers would have no reason for suddenly deciding at 23 weeks and 5 days that their baby should have active intervention.
I am sure that the physicians who resuscitate 100% of the babies at 22 weeks, and those that resuscitate none of them, all think they practice shared decision-making. But clearly if there are no babies being resuscitated, (once there are significant numbers of mothers in the data) then the values of the physicians and the care team are being imposed on the families. If the decision was truly shared, then there would be at least a few who occasionally received active intervention.







Pingback: Excellent blog post about when to resuscitate preemies | They don't cry
Great logical argument !, once again highlighting the well known limitation of gestational age assessment and I wonder why we keep discussing this topic in terms of gestational age ! (including the NICHD outcomes). I think the best objective criteria we all can access easily is the birth weight. If the birth weight is > 400 g (for 22-23 weeks estimated GA), then I feel, they all deserve a ‘trial of life’. If the estimated GA is 24 weeks and above, then trial of life should be offered irrespective of the birth weight.
Babies with BW > 400 g and borderline viable GA (22-23 weeks), the ‘trial of life’ will tell us whether they have the physiological maturity to survive, most of them self-declare this in the first 1-2 days itself. If we have enough time prenatally, then we can discuss the specifics of resuscitation and facilitate the parents to reach some consensus.
Thanks Keith, i would simply add a sentence to your final paragraph – That if shared decision making is the the case, then no center should also have 100% resuscitation, just as no center should have 0. Saying that, the comment above about giving 100% of them at 400 grams a trial of life is also not shared decision making. True?
Absolutely, I do think that the “trial of therapy” should be a real option, when there is a realistic chance of success. How you define realistic should definitely be based on an evaluation of the parents values, their hopes and wishes, and an honest calculation of the probable outcomes.
I think a universal imposition of a precise cutoff for any of those calculations is not where we should be going. So always resuscitating babies of (for example) 400 grams, would not respect shared decision making. Some babies of that size would have such low chance of survival that offering comfort care would be consistent with many families values (and certainly with mine). There are other (female, growth-restricted 24 week best-guess gestational age, steroid complete, singleton) 420g babies where the chances are good enough that many families would find a trial of therapy consistent with their values (and also with mine).
This is one thing that I think we should examine in more detail, when the shared decision making includes a share on the part of the care team, how much should the values (rather than just the knowledge and expertise) of the neonatologist and their teams play a part?
I don’t think we can avoid there being a part for those values, but they should be explicit. Right now they are hidden, in large part, in how we talk about these issues. But when we examine rates of active intervention, and their variations, they become very clear.