To reiterate, the PEPaNIC trial, and a subgroup analysis of the newborn group, mostly babies who needed surgery, showed that babies receiving early TPN had more nosocomial sepsis, longer assisted ventilation and longer PICU stays compared to the late TPN group, who delayed for 7 days.
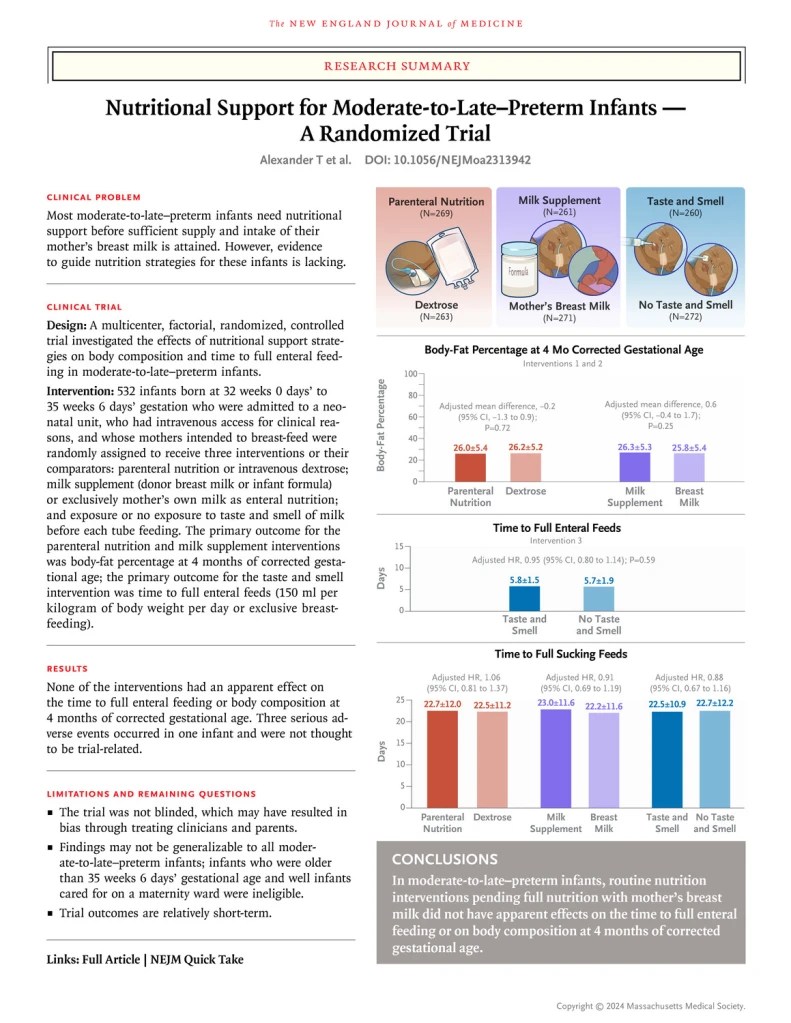
The new trial has a multi-coloured summary :
To be eligible for the study the baby had to be admitted to an NICU, have an IV access in place, and have a mother intending to breast feed. I will focus on the IV amino acid vs glucose solution arm of this complicated factorial trial, in which babies after randomization received either an amino acid solution or a glucose solution until they were full enterally fed. IV lipid was added, in either group, at the clinicians’ discretion, and the composition of the amino acid solution was according to local hospital practice. The actual intravenous protein intake averaged 1 g/kg/day over the first week, but, as many were stopped prior to 7 days of age, I can’t tell how much was being prescribed on the days while they were actually receiving the intervention.
The 269 babies in the TPN group over the 1st week of the study therefore received more total protein, averaging 2.6 g/kg/d, compared to 1.8 for the 263 babies in the glucose group. During week 2 the intakes were identical; almost all in both groups were off IV fluids. Fat intakes were also higher during the 1st week at 3.4 vs 2.8 g/kg/d, but carbohydrate intakes were a little lower at 8.6 vs 9.2 (2.8 vs 3.3 of which was intravenous). All of the enteral nutritional intakes were very similar between groups.
The time to full enteral feeds, and therefore discontinuing the TPN intervention, was a mean of 5.7 days in each group.
The primary outcome of the study was a measure of growth at 4 months of corrected age, that is fat-free mass. This outcome was identical between the groups at 4.9 kg.
There were 3 times as many episodes of culture-proven late onset sepsis with early TPN, and 3 times as many episodes of ‘probable sepsis’. Which sounds dramatic, but the actual number of each was 3 vs 1, and 3 vs 1, which, of course, is not statistically significant. Or, in other words, it might have been a chance difference, except that it is consistent with the other data which are accumulating. Other outcomes such as duration of hospitalisation were identical between groups, and most were not on respiratory support, so one cannot comment on duration of such support as an outcome.
In this low-risk group for serious adverse events, there was no sign of an advantage of receiving amino acid solution while enteral feeds were being established. There is a hint of adverse consequences.
Although the trials are not directly comparable, they have in common relatively mature newborn infants, and early versus delayed, or no, intravenous amino acid solutions.
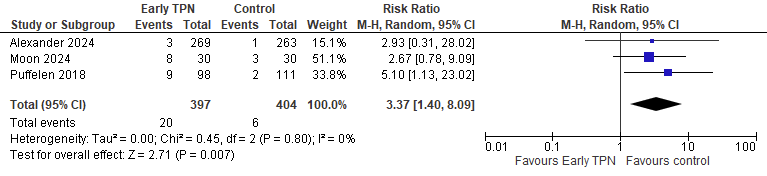
They also have in common, as results, a difference in hospital acquired infections between groups. In the PEPaNIC results there are several different categories of infections, including airway infections which are notoriously difficult to define in newborn infants. So by extracting the culture-positive blood or CSF infections from the 3 trials, and putting them in a meta-analysis (I know this is questionable, but to give an indication rather than bullet-proof data) you get the following Forest Plot:
Alexander 2024 is the new publication of the DIAMOND trial, Moon i2024 s the trial I described in the last post, and Puffelen 2018 is the newborn subgroup of PEPaNIC.
Please note, this is not a formal systematic review or meta-analysis, just an idea of the similarity of the data between the trials, which have major differences. In particular, the babies in Alexander were a very low risk group, and more immature.
But, given the lack of any indication of benefit from early TPN in such babies, I think we must reconsider that approach. Waiting until the babies are clearly in need of parenteral nutrition, after several days, seems to be consistent with the available data. Early TPN is not indicated for babies at or near term, or for late preterm babies who are likely to be fed shortly. Exactly how long to wait, and what the indications are for TPN in such babies, will require more research.
There are 2 new trials addressing different aspects of the questions surrounding what to do about TPN for this group of babies.
My readers may remember my post about the PEPaNIC trial, which showed that there were disadvantages of early TPN, compared to TPN starting after 7 days of ICU among PICU patients. And the subgroup analysis which showed that the same results applied to the newborn infants in that trial, who were mostly babies who needed surgery. Babies receiving early TPN had more nosocomial sepsis, longer assisted ventilation and longer PICU stays.
The first of the 2 trials I wanted to discuss is a smallish single centre trial, with some similarities to PEPaNIC. (Moon K, et al. Early versus late parenteral nutrition in term and late preterm infants: a randomised controlled trial. BMJ Paediatr Open. 2024;8(1)) 60 babies of at least 35 weeks, admitted to the NICU, who were expected to not be fed for at least 3 to 5 days were randomized soon after admission to either start immediate TPN or to wait until day 6. The trial is clearly too small for clinical outcomes to be the primary, so the primary outcomes were serum phenylalanine concentrations (to see if the babies were tolerating the amino acids they were given) and F2-isoprostane (as an index of oxidative stress).
The early TPN babies received more protein and more total calories during the randomized period, but by day 8 there were no differences in intakes. TPN babies were more likely to have mild hyperglycaemia (>8.3 mmol/L), both groups had a lower body weight z-score at discharge than at admission, and the fall was greater in the late TPN group (-1.0 vs -0.6).
The publication states “all other clinical outcomes were similar between groups”, but I beg to differ! In the supplemental materials we find : 8/30 early TPN babies developed a hospital acquired infection, compared to 3/30 late TPN babies, 27% vs 10%, or more than double. In the published protocol we note that these are culture-positive blood or CSF infections. Duration of NICU stay was 5 days longer (21 vs 16) with early TPN, and total duration of hospitalisation was 4 days longer, 23 vs 19 d. Duration of respiratory support was 16 hours longer among babies who were on such support. There was also twice as many babies with hypoglycaemia in the early TPN group (4 of them vs 2)
Of course, the authors had to very careful to not make too much of those differences in such a small trial. They are, relatively speaking, large differences, but could have been due to chance. What is striking is that the differences are all consistent with what PEPaNIC showed, (apart from hypoglycaemia, which was more common in the late TPN group in PEPaNIC).
The primary outcomes did show a difference in phenylalanine levels, which were 30% higher in the early TPN group during the randomized period, but almost identical afterwards. Isoprostane levels were similar between groups throughout.
The practice of starting very early TPN was based on a physiologic rationale for the very preterm infant, with the desire to reduce catabolism among infants with very limited energy and protein stores at birth, and evidence that this physiologic goal was attained by immediate, or very early TPN. The practice has slowly spread to other babies in the NICU, and TPN is often started early among other infants, for whom there is no evidence of benefit. Among such infants, however, there appear to be negative impacts, and there is no clear evidence of benefit.
I think that term and near term babies, admitted to intensive care units, who cannot be full fed immediately, can wait several days before TPN is considered. Whether we wait 3 days or a week or even longer is uncertain, and will require larger studies, the current state of knowledge is that there is no need to hurry.
The title of the post sneakily did not mention that I am referring to a study in a specific subgroup of babies, the paper is a report of an RCT in newborn infants who had heart surgery. Yildirim MI, et al. The Impact of Nasal Intubation on Feeding Outcomes in Neonates Requiring Cardiac Surgery: A Randomized Control Trial. Pediatr Cardiol. 2024;45(2):426-32. Full term babies who needed intubation for cardiac surgery were randomized to an oral or nasal intubation group, 70 babies were included, and 3 of the nasal group actually had oral intubation. There are a couple of problems with the study, the 3 babies randomized to nasal intubation who couldn’t be nasally intubated were analyzed as oral intubations, in other words there was not an intention to treat analysis, also the outcome variable had 3 possible values, completely orally fed, or needing an NG tube, or having a gastrostomy, but each outcome was analyzed independently.
All but one of the nasally intubated babies were fully orally fed at discharge with the other needing NG feeding, compared to 28 of the 37 who were orally intubated being full fed by mouth, with 3 going home with an NG tube, and 5 with a gastrostomy. The authors do mention that eliminating the 3 babies from the nasal group who were orally intubated made the results “non-significant” for full oral independence.
I don’t think there is another similar study available, previous randomized comparisons of oral and nasal intubation have not examined feeding outcomes to my memory; but this sounds like a major advantage for families of nasal intubation in this group of babies.
It would be interesting to see the impacts on oral feeds in preterm infants of route of endotracheal intubation. The tiniest preterm babies, who have the most feeding problems, cannot in my experience be nasally intubated at birth, usually the nostril will blanche around the tube, so I no longer even try below about 800 g. I do think there is a role for an RCT in other term infants and in preterm infants with prolonged intubation. I don’t think a day or two of intubation at 29 weeks (for example) is likely to have differential impacts on long term feeding outcomes between oral and nasal intubation. But babies with severe lung injury, ventilator dependent, and especially those approaching the PMA where oral feeding skills start to progress, might well benefit from having no oro-tracheal tube in place.
There is one older study, by the group in Rhode Island (Bier JA, et al. The oral motor development of low-birth-weight infants who underwent orotracheal intubation during the neonatal period. Am J Dis Child. 1993;147(8):858-62), led by the amazing Betty Vohr, that showed that preterm babies who had prolonged oral intubation had poorer sucking skills at term, and even after 3 months corrected age. It seems likely that oral endotracheal tubes do have an impact on oromotor development, it is unclear in the preterm whether nasotracheal intubation is preferable in this regard, as there are no coparative data I am aware of. Prolonged nasotracheal intubation can lead to distortion of the nose in smaller preterm babies, so it would warrant, I think, a good RCT to determine which route is preferable. What I would do would be to randomize very preterm infants who arrive at 30 to 32 weeks PMA, who look like they will need prolonged intubation, to either oral or tracheal intubation until their final extubation. The development of their feeding skills could then be followed over several months, in addition to investigating whether there were impacts on unplanned extubation, nasal growth and injury, oral/palatal groove development, pulmonary injury, time to discharge, etc.
This also makes me wonder whether there is a difference in feeding development and progression between oro- and naso-gastric tubes. As far as I am aware there are a few small RCTs, which have looked at things like pain scores during insertion, cardiorespiratory stability, and feeding tolerance. One did show that babies with orogastric tubes generated lower sucking pressure than those with nasogastric tubes, but no data about progression of feeding was given.
I don’t know of any trials that have looked at whether there is an adverse impact of oral feeding tubes (compared to nasal tubes) on development of feeding competence, or duration of hospitalisation (which is often prolonged by feeding problems) and yet it is an extremely common practice, with potential important impacts that would be of interest to families, I’m sure.
Feeding problems, slow development of feeding competence, oral aversion, and various difficulties feeding are very common. Waiting for full oral feeding is commonly the last thing that keeps a preterm baby hospitalised. After discharge, one of the commonest concerns of families are those feeding issues, yet there is next to nothing in terms of good quality evidence to help improve those problems. Even something as simple as whether we should use oral or nasal endotracheal tubes, or oral vs nasal gastric feeding tubes has never been well studied for impacts on feeding development.
The field is wide open for young investigators to perform studies that could have a big impact on clinically important outcomes that concern parents.
Previous studies have shown that vitamin A supplementation can reduce the frequency of BPD, but the practice has not become widespread. In part, I think, it is because repeated intramuscular injections of vitamin A are the route that has been studied, and there is an understandable reluctance to subject the babies to this.
If you could ensure adequate vitamin A status by another route, and show efficacy, then perhaps that would change the common approach.
In other words this was an RCT comparing an additional 6000 u/kg/day of vitamin A to an additional 1000 u/kg/day, on top of what was in their nutrition. Breast milk vitamin A is very variable, and varies from somewhere around 300 iu/100 mL in colostrum down to 60 iu/100 mL in mature term breast milk. Breast milk fortifiers tend to give close to 1000 iu when mixed with 100 mL of breast milk in the usual fortification to 87 kcal/100mL. In other words, a preterm baby, on 165 mL/kg/d of breast milk with standard fortification, should get somewhere around about 1700 iu/kg/day of enteral vitamin A.
The study found absolutely nothing. Every single outcome was close to identical between the 2 groups, BPD, and all the other 3-letter outcomes were very similar. Of note, the relative risk for NEC was 0.7, which reflected 6% with the high dose compared to 8% with the less high dose, but this was entirely consistent with a chance effect (95% CI for the RR 0.42-1.18). Which illustrates how many babies would be needed to prove a clinically important reduction in NEC in a prophylaxis RCT.
About half of the babies at each of 3 time points (before, during, and at the end of the trial) had serum retinol concentrations measured, and they were very similar between the 2 groups. It is likely that the mothers in this study were not malnourished, so it is likely that the vitamin A intakes from the basic nutrition that were calculated by the investigators have some accuracy, and they were indeed at least 1500 iu/kg/day in both groups even before the supplements were added.
A previous meta-analysis suggested that vitamin A supplementation was only effective among babies with a baseline vitamin A intake <1500 iu/kg/day. With another suggesting that it was only effective in lower risk babies.
This new RCT confirms that enteral vitamin A supplementation at 6000 iU/kg/day compared to 1000 iu/kg/day in addition to that provided by breast milk and fortifier (which the majority of babies were receiving) or formula, has no impact on BPD, in a population where mothers are likely to have diets sufficient in vitamin A.
As I have described, the control babies did get an extra 1000 iu/kg/day vitamin A already on top of their nutritional intake. I have never done that, I guess it must be frequent in Germany, where most of these centres were located. It probably isn’t necessary, the 1500 or so in regular fortified breastmilk or preterm formula may well be enough.
By now, my gentle readers probably know that I don’t think BPD is a useful measure of lung injury. In the supplemental material for this trial they describe other variables, such as duration of oxygen therapy, and duration of ventilatory support, but I can’t find any data. There have been other studies showing no impact on BPD, but nevertheless an impact on post-discharge clinically important outcomes (such as the SUPPORT trial CPAP arm), if there is funding, longer term follow up would be interesting, but to be honest, I would be very surprised if there was any difference in respiratory outcomes of importance to parents after discharge. Vitamin A is essential for lung growth and development, but once you have enough giving more doesn’t improve them further.
For those who are unaware, the Silverman Lecture is an annual honour bestowed by the AAP. A neonatologist who has made. or is making, major impacts in neonatology is asked to deliver the lecture. Bill Silverman was one of the early pioneers of neonatology in the USA, and was very outspoken about the need for evidence-based practice (having performed some of the earliest RCTs in neonatal medicine himself).
This years lecturer was Annie Janvier, and, for the first time ever, a second speaker was invited to collaborate on the presentation, a mother that Annie (and I) have worked closely with, Rebecca Pearce. Rebecca and Annie have both had extremely preterm infants, Rebecca recounted, at the start of her part of her talk, that she had twins Lily and Maren at 25 weeks. Lily died within her first few days of life of early onset septicaemia, and Maren, who also had EOS, survived. Rebecca and her husband have written about their experiences with the pre-discharge MRI, and they have become valuable members of our parent resource team at Sainte Justine. One particularly moving part of her presentation was a slide which listed on one side all of the diagnoses that Maren has had from doctors (including various delays and executive function disability), in the middle was a picture of a lovely smiling 14 year old girl, and on the other side a list of her characteristics as seen by her family, “caring”, “warm”, “bubbly” “hard worker”.
Annie’s presentation recounted, a little, our course with Violette, including this briefly shown picture of me doing kangaroo care in the NICU!
It also included pictures of Violette in the PICU, intubated after her tracheal reconstruction at the age of 15. She noted that Violette did not have “BPD”, as she came out of oxygen a couple of days before she hit 36 weeks, but that she certainly had respiratory fragility, and had serious upper airway problems, receiving several courses of steroids for stridor with signs of obstruction during her first few years of life. An outcome which has rarely or never been described in neonatal follow up studies, but which is well known to paediatric ENT surgeons. (As you can see, the image is from a day or two after the surgery when “ça va mieux”, things are going better).
Annie described the work of the “Parents’ Voices” project, which was created to “Engage Parents to Co-create” definitions of what are important outcomes of neonatal care, on which Rebecca is a co-investigator .
One of Annie’s slides, which illustrates that our current measures of “NDI” don’t reflect what parents think about their children, was derived from data in one of the Parents’ Voices publications. It showed that, when we categorize infants as having No NDI, mild-moderate NDI, or severe NDI, parents often disagree with us, a disagreement that increases the more “impaired” we think their child is. Only 12% of parents whose child was categorized as sNDI agreed that their child was severely impaired, a third of parents of such children don’t find them impaired at all. On the other hand there were 25 parents who found their child severely disabled, 22 of them were classified sNDI by the CNN definition, but 3 had either no or mild NDI.
Annie listed some of the publications from the project to date (and there are more to come!):
As you can see I am co-author on some of them, being a collaborator, rather than a member of the core group. I am proud to be associated with this group who are making great strides in re-defining what outcomes are of importance to families. The CNFUN is incorporating many of the measures that parents find important, for which validated instruments exist, into the national follow up database.
Here are the 2 Silverman Lecturers on the big day:
The lecture was greeted with a standing ovation from the audience,
This was followed by a Q&A session, which was generally thoughtful and appreciative. Unfortunately it ended with a comment from a retired neonatologist who said two things: Firstly, that quality of life is subjective, so shouldn’t be used as a primary outcome. I’m not sure I agree, you can measure quality of life just as well as you can measure the incredible complexity of child development; the person posing the question led a few very high quality studies (2 of which I was involved in), in which, unfortunately, like so many others, we dichotomised the richness of children’s developmental progress into “pass” or “fail”, “NDI or “no NDI”. I would agree, however, that you shouldn’t divide quality of life into 2 categories, of good or bad QoL. But in a sense, unless an intervention improves some aspect of QoL then what value is it? Secondly, they also stated that it is important that there is link of scientific plausibility between the intervention and the outcome. That is self-evident, and indeed what the Parents’ Voice project is trying to do is to develop more appropriate plausible outcomes: Parent-Important respiratory outcomes for respiratory interventions, Parent-Important developmental and neurological concerns for Neuroprotection studies.
The outcomes that are important to parents are also, often, the outcomes that are important to society as a whole, and that often have an impact on medical resource use. To take an example from the previous post, it matters little to anybody if a baby needs a few more days of oxygen while they are hospitalised. What matters to parents, and has an impact on society and resource use, is if discharge is delayed by pulmonary concerns (such as oxygen dependence), or if the baby needs oxygen at home, or has recurrent admissions post-initial discharge, or has difficulty feeding because of tachypnoea, etc. Until we start to measure such things, we have little idea if our interventions are having an impact on outcomes that really matter.
There was a hiccup yesterday, I was writing the part 2 and it suddenly got posted as just the title, and the entire post disappeared. I had to start all over (which has never happened before, there are usually automatic and frequent manual backups, but they all vanished). So as I rewrite it, here is an interim, a link to a video about someone I appreciate enormously.
One of the true giants of neonatology, and one of its true gentlemen, Alan Jobe, was honoured at the meeting, being given the Howland Award. Alan has made a huge impact on the care of babies, his achievements are too many to fit in a short video, but this link will take you to a 7 minute video. A full description of what he has done to improve neonatal care and help babies around the world would take far longer than 7 minutes!
This trial was a modestly sized RCT of low dose diazoxide for treatment of persistent or severe hypoglycaemia in newborn infants of at least 35 weeks gestation. I say “modestly sized” as a descriptor, not a criticism, because I think this trial is potentially very important. It included 75 babies admitted to the NICU in the first week of life who had ≥3 episodes of blood sugar <2.6 mmol/L in a 48 h period, or a persisting episode <2.0 mmol/L despite gel on 2 occasions, or any episode with a blood sugar <1.2 mmol/L, AND ongoing treatment for hypoglycaemia, which meant IV dextrose, continuous or frequent feeds (≤2 hourly), inability to wean formula
Babies were randomized to either 5 mg/kg of diazoxide followed by 1.5 mg/kg q12h, or placebo.
After the first 2 doses further doses were adjusted according to the following schema, the doses are given in mL/kg as it was a masked trial, but the drug was concentrated so that 1.5 mg/kg was 0.15 mL/kg.
The primary outcome was a complicated one, evidence of stabilised glucose metabolism, as shown by: established enteral bolus feeds (either breast or bottle); no IV fluids for at least 24 hours, and all glucoses in range (2.6 to 5.4 mmol/L with at least 4 of them prior to a feed).
The primary outcome was shorter with diazoxide, but not statistically different between groups (2.8 days with diazoxide cf 3.7 days in controls). Nevertheless, there seemed to be some major advantages of being in the diazoxide group. Only 2 of the diazoxide group had a mild hypoglycaemia after the loading dose was given, whereas, in the control group, 53% had ongoing hypoglycaemia, 21% had recurrent or severe episodes, 16% had hypoglycaemia after initial stabilization, 29% had study drug dose increases, and 3 required open label diazoxide to achieve control.
They redefined the outcome variable after the study (always a dangerous thing to do) to be a bit simpler, “Time to resolution of hypoglycaemia AND full enteral bolus feeding AND no IV fluids for ≥24 hours”, and that was substantially shorter in the diazoxide group, who had no adverse effects (2 babies with blood sugar in the high normal range) and, importantly, had many fewer heelsticks, a median of 15 instead of 20. In comparison many control babies had repeated and/or severe hypoglycaemia after the initiation of the trial: 53% had ongoing hypoglycaemia, 21% had recurrent or severe episodes, 16% had hypoglycaemia after initial stabilization, 29% had study drug dose increases and 3 required open label diazoxide to achieve control.
They also noted that babies had an IV infusion for a shorter time, and there was no recurrence of hypoglycaemia when the diazoxide was stopped. I think this warrants further investigation, especially in the severe group, less than 1.2 or multiple samples <2.0. And always remember that bedside glucometers are very inaccurate in the hypoglycaemic range, often over-diagnosing hypoglycaemia, as yet another study showed, presented as a poster in this meeting. The Auckland group have always used reliable methods in their studies, with high quality lab analyses (usually with a blood gas analyser or the EPOC device), which of course, have to be available very rapidly for this problem.
The ESC-NOW trial was a multicentre investigation of using ESC (Eat Sleep Console) instead of the Finnegan scale for neonatal opiate withdrawal. This secondary analysis showed that maternal buprenorphine treatment was associated with much less neonatal morphine use, and shorter medication use and shorter hospitalisation than maternal methadone treatment.
The ESC approach was advantageous in both groups, shortening hospitalisation from 11 to 7 days in the buprenorphine group and from 17 to 10 days in the methadone group. Need for medications in the babies was decreased from 39% to 15% with ESC in the buprenorphine group, and from 63% to 31% in the methadone group. As far as the impacts on the baby, it is clear that using buprenorphine is preferable to methadone during pregnancy. For an individual mother, of course, there may be enormous numbers of other considerations.
This was a single group study of the use of High Frequency Oscillation with the Draeger VN500 in pressure and then volume guarantee mode. The study was all funded by Draeger, and seems to have been done largely to try and get approval as a medical device in the USA. Subjects were 24 to 30 weeks infants in the 1st 4 days of life who still needed more than 25% oxygen after surfactant with an MAP of 7 or more. Initially the MAP was increased by 2 when the baby was switched, and the initial pressure amplitude was 15-20 cmH2O, which was adjusted by eye, looking for a chest jiggle that appeared right! TcCO2 was used and early blood gases to avoid hypocapnia.
Although not randomized, there was a concurrent control cohort, and outcomes were all very similar to those who stayed on conventional ventilation. Except for pneumothorax which was 4% in the HFO group, and 11% in the conventional group. 11% seems very high to me, after surfactant there are usually far less than that, but not knowing how the control cohort was enrolled makes it difficult to comment.
CO2 fell after the change in ventilation mode, with a mean about 45 mmHg at 2 hours, and a SD of about 4, which means that a mean -2SD is about 37, and there will be occasional babies with more severe hypocapnia. After stabilisation the babies were switched to Volume Guarantee Mode, which, just as in conventional ventilation means that the ventilator adjusts the pressure to give the volume that you set. The mean volume used was close to 2 mL/kg.
This is similar to previous data, that, at 10 Hz, the average volume required is close to 2 mL/kg. Because of those prior findings, and the occasional occurrence of severe hypocapnia in our babies after switching to HFO, we now initiate HFO with Volume Guarantee and a volume of 2 mL/kg. Since starting that approach we have had no severe hypocapnia: I think that makes much more sense than trying to evaluate if the chest is vibrating the right amount. We also try to keep all the preterm babies on 10 Hz, people get confused by the changes in high frequency tidal volumes and DCO2 when you change frequency, so keeping them all at 10 Hz simplifies things. However, with the VN500 you often can’t achieve your desired tidal volumes in larger babies at 10 Hz, and often have to reduce the frequency to 9, 8, or even 7 Hz, to get adequate ventilation.
2 mL/kg is however, just a starting point, some babies will still be mildly hypocapnic, on the first blood gas, which should be done rapidly after switching to HFO, and will need volumes eventually as low as 1.2 mL/kg, others may need volumes as high as 3.5 or occasionally even more.
Many of you will remember the MINVI trial of cord milking for non-vigorous term infants. That trial had a null primary outcome, but re-analysis using the DOOR methodology showed that short-term outcomes were improved with cord milking compared to immediate clamping.
As you can see from this illustration by Satyan, several outcomes of interest to parents were improved by milking, and there were no adverse effects.
At 2 years of age the babies were evaluated with the Ages and Stages Questionnaire, and with the Modified Checklist for Autism in Toddlers (MCHAT). The proportion of babies with abnormal scores on each domain of the ASQ-3, was identical in the two groups. There were no evident outcome differences between groups. I think this means that cord milking in such babies should be routine, having fewer babies with moderate to severe HIE and/or needing Cooling are substantial benefits. Especially as there were no adverse impacts, and the babies also have a higher red cell mass, and therefore higher iron stores, it may be that other benefits will show up later, as has happened with the term delayed clamping trials, where higher haemoglobin led to better very long term outcomes at 4 years, despite no difference at 1 year.
The Darbe trial was a multicentre RCT of darbepoetin among over 640 very preterm infants with the primary outcome being based on an interest in determining whether there was neuroprotection, it hasn’t yet been published in full, but seems to have had no impact on the primary outcome. 23 to 29 weeks infants were included, and the primary outcome is neurological and developmental findings at 2 years corrected age.
P
•650 infants born 230/7 to 286/7weeks’ gestation •Enrolled ≤24hr of age between 2017-2019 (f/u through 2022)
I
•Darbepoetin 10μg/kg weekly (IV or SC) through 35 weeks’ PMA
C
•Placebo (IV) or sham injection (SC)
All
•Parenteral or enteral iron supplementation per study guidelines •Restrictive protocol for red blood cell transfusions
O
•Primary: Bayley III composite cognitive score at 22-26 months •Secondary: Multiple pre-specified outcomes
The presentation didn’t have a slide saying “not to be shared” so I can copy the above data from the pdf, some of the others had such a slide, so I haven’t cut and pasted any figures or slides for some presentations.
Darbepoetin reduced the number of RBC transfusions compared to controls, the mean transfusion number was 1.9 (2.8) vs. 3.3 (3.6), and the proportion who never had a single transfusion was 46% compared to 24%.
The short term respiratory outcomes showed a reduction in grade 2 or 3 BPD with darbepoetin compared to control, from 46% to 34% among survivors; mortality was similar between groups. They performed a mediation analysis to show that it was possible that the reduction in BPD was mediated by the substantial reduction in transfusions.
Although they have gone to great statistical effort to show the potential mediation of the reduction in BPD by a reduction in transfusion, we should keep in mind that the TOP study, in which there were far fewer transfusions in the low hemoglobin group, showed no difference in BPD, or any other index of lung injury.
Short term respiratory outcomes that are of more interest to parents were, however, not different between groups. The proportion of babies going home on oxygen was the same, 37% vs 38%, and the proportions on respiratory medications at discharge were also very similar. Among respiratory outcomes at 2 years of corrected age, 5% in each group were still on oxygen, and 2% on respiratory support, about 1/3 were getting respiratory medications, and 1/5 had been readmitted to hospital for respiratory complications. There was no difference between groups in any of these outcomes.
Darbepoetin therefore had some effect on respiratory adaptation in the NICU, with babies in the active treatment group needing 7 days less of oxygen supplementation, and 7 fewer days of positive pressure, perhaps having something to do with the transfusion need. But no important impact on any outcome that matters to parents, or, indeed, matters to society in terms of health care resource needs.
Thanks to the NRN and Dr Jensen, for providing yet more evidence that “BPD” is of little value as an outcome variable in clinical trials.
Although there was a major reduction in BPD in this trial, it was because control babies needed oxygen or positive pressure for a little while longer, and thus they were more likely to still be in oxygen at 36 weeks PMA, but, as I already noted, none of the outcomes that we have shown to be concerns of families were affected. I think an ordinal outcome variable including several clinically important signs of lung injury would be much more useful for the future. Such an outcome should be co-constructed with parents (and former preterms, perhaps) and would probably include: discharge delayed because of respiratory difficulties; home oxygen after 40 weeks PMA; respiratory medications at discharge; home gavage feeding after 40 weeks PMA. Somewhere in there should also, be the rarer outcomes of prolonged ventilation past 40 weeks, tracheostomy, and so on.
If we keep using “BPD” there is a real risk that interventions that have no major real impact on lung injury, such as darbepoetin, may be widely used to improve pulmonary outcomes, which, based on these data, would be a big mistake. In contrast, using darbepoetin to reduce transfusions may indeed be something that appeals to parents. I think that being able to avoid transfusion might be something that parents would value, if there are no adverse impacts of the medication, which seems to be the case.
As usual the PAS meeting was packed with neonatology. The App was even worse than last year, crashing frequently on many peoples’ phones. It was completely useless for the posters, as they were listed by number, and the different sessions all started with #100; so there might have been 3 posters with the same number and no indication of which day they were on.
The organisers also decided to not have any indication of what subjects were in various areas of the poster session, so you might accidentally happen upon a group of posters about breast milk and breast feeding, for example, but there wasn’t any way to know that such a group existed, or how to find them. As there were several hundred posters in each session, it was impossible to actually find the things that interest you. If I wanted to see the posters about neonatal respiratory care, I just had to wander around the huge room and try to find them, the App didn’t help at all.
Sunday morning was very interesting, with Neonatal Clinical Trials 1 followed by the Silverman lecture given by Dr Annie Janvier then Neonatal Clinical Trials 2. Unfortunately there were other interesting neonatal things going on at the same time, which had tiny participation, a session on BPD and another on caffeine would have been super interesting, but I would guess had almost no-one there, as the Clinical Trials sessions were packed.
As for those Clinical Trials, I will outline a few of them here and give a link to the protocol if one is published, and may well return to them with a longer post when they are actually published. One of them was the Video-Laryngoscopy trial that I have already posted about. In no particular order the others were :
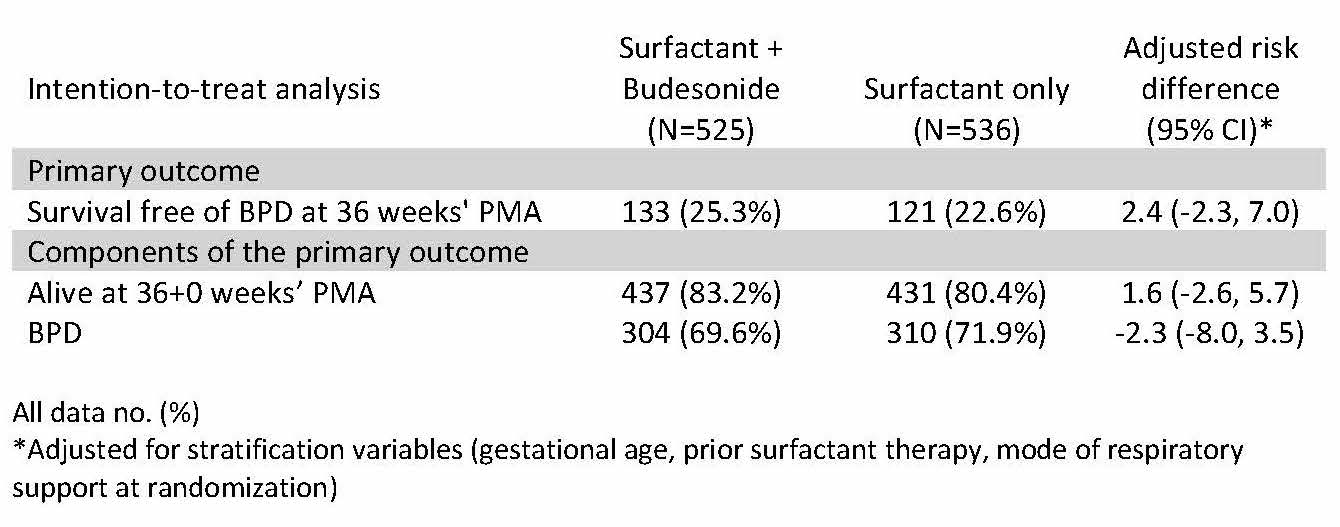
The PLUSS trial
The PLUSS trial showed that budesonide is not a plus when added to curosurf. Many of you will know that previous work, including moderately large trials from Taiwan, have suggested a reduction in early signs of lung injury when initial surfactant dosing was mixed with budesonide, comapred to budesonide alone. This trial randomized infants <28 weeks receiving surfactant either by intubation or LISA/MIST, and followed the babies until discharge.
As you can see there was no impact on either BPD at 36 weeks, or survival to 36 weeks. I think it is very unlikely that any longer term follow up will show a benefit from the budesonide, although there may be a risk of neurodevelopmental adverse impacts form this potent steroid, a small proportion of which is absorbed. There was no subgroup that appeared to have any benefit. A recent observational study has suggested that the budesonide only seemed to help the larger babies, perhaps that is the difference to the prior positive trials, which included many larger infants.
IBUPAR
The IBUPAR trial was a multicentre Spanish trial including preterm infants <30 weeks with a “haemodynamically significant” PDA, to either Ibuprofen or Paracetamol (=acetaminophen), which was diagnosed on average about 3 to 4 days of age. I found it odd that this was being presented, as the sample size is 274, but only 134 have completed the trial and 111 completed the treatment, nevertheless the data from an interim analysis have been unmasked in order to be presented at PAS. The primary outcome is closure of the PDA, which occurred in 60% with ibuprofen, and 40% with paracetamol. By the time of discharge most had closed in both groups, but it was 85% in the ibuprofen group and 70% with paracetamol. Acute Kidney Injury was much more frequent with ibuprofen, 16% vs 5%, but I am not sure what the diagnostic criteria were for that diagnosis, whether it was a transient oliguria, or persistent increase in creatinine, or some combination. There were no major differences in NEC, BPD, IVH, ROP or mortality. This shows I think that it doesn’t matter much if you give a less effective therapy to close the PDA, the babies turn out just as well despite having an open PDA.
There were two trials of prolonged use of caffeine in the preterm.
The MOCHA trial
The first was the MOCHA trial, which unfortunately. despite the name, did not give the babies chocolate along with their caffeine. In this trial 827 moderately preterm babies (29 to <34 weeks GA) who had received caffeine for clinical reasons, and had arrived at 33 to <36 weeks PMA, with a plan to stop their caffeine, were randomized to continue caffeine citrate at a dose of 10 mg/kg/day or placebo, with the plan to continue until and beyond discharge, for a further 28 days at home. The primary outcome was the number of days of hospitalisation, the idea being, of course, that less apnea, and fewer hypoxic events will lead to earlier discharge. There was no real difference in the primary outcome, which was slightly shorter in the placebo group, and identical after adjustment. Days to “physiologic maturity” (which meant apnea free, full oral feeding and stable in a crib) was also identical. Caffeine was having an effect, however, the caffeine group babies had fewer apneas, it was 2 days faster for them to be 5 days apnea free, but in the end it wasn’t apnea that kept most babies in hospital but feeding issues. There were no adverse effects, so in terms of duration of hospitalisation, caffeine is likely to only have an impact in the subgroup who are having persistent apnea.
The ICAF trial
On the other hand, the ICAF trial enrolled more immature babies <30 weeks GA at birth, who had arrived at 32 to <37 weeks and were about to have their caffeine stopped. Within 3 days of caffeine being stopped they were randomized to caffeine or placebo at the standard dose, but when they reached 36 weeks the dose was doubled to 20 mg/kg/day of caffeine citrate. The babies were on recording pulse oximeters until 44 weeks, and stayed on caffeine or placebo until 43 weeks. 160 babies were in the study, and these are the post-randomization findings.
Characteristic
Placebo N= 78
Caffeine N= 82
P-value
Clinical caffeine
3 (3.8)
3 (3.7)
0.95
Supplemental oxygen
14 (17.9)
4(4.9)
0.009
CPAP, BIPAP or High Flow NC
7 (9.0)
2 (2.4)
0.07
Mean (SD) PMA (weeks) at discharge*
38.5(2.2)
37.7(2.2)
0.04
Mean (SD) weight gain (g/day)*
38.5(25.3)
29.2(12.7)
0.004
Median (min – max) days from randomization to discharge)**
27 (21 –32)
17 (15 –23)
0.001
In these more immature babies caffeine did shorten hospitalisation, and improved their respiratory course, not just in terms of apnea, but by keeping them off oxygen or respiratory support. The oximeters showed dramatic effects on intermittent hypoxia, which continued to be significantly different until 42 weeks.
I think the big difference between the two trials is the less mature group enrolled in ICAF, who have more IH for longer, and have more lung disease.
We already know that caffeine metabolism changes at near to term, and levels are very low on the standard dose, so I think the increased dose was a good idea in ICAF. But I don,t think it would have made much difference to MOCHA as it wasn’t apnea, or IH that were keeping the babies in hospital.
Long term follow up will be important for both trials, and ICAF2 with a larger sample size is certainly warranted based on this information.
I posted about the short term results previously, it was an RCT of early closure of the PDA with ibuprofen that had basically a null result. The infants were followed at 2 years of age, with parental report of their development using a scale called PARCA-R, unfortunately the outcome was dichotomised into those with moderate or severe “neurodevelopmental impairment” or without. There were slightly more overall deaths with ibuprofen, and slightly more so called “impairments”, most of which I presume was slower development, in the controls who survived.
Longer term respiratory outcomes were also presented, including duration of oxygen treatment from randomization to stopping oxygen, and a composite of respiratory morbidity, the definition of which is shown in the legend to the figure below. It shows not a hint of any difference.
Trial of Prolonged CPAP therapy
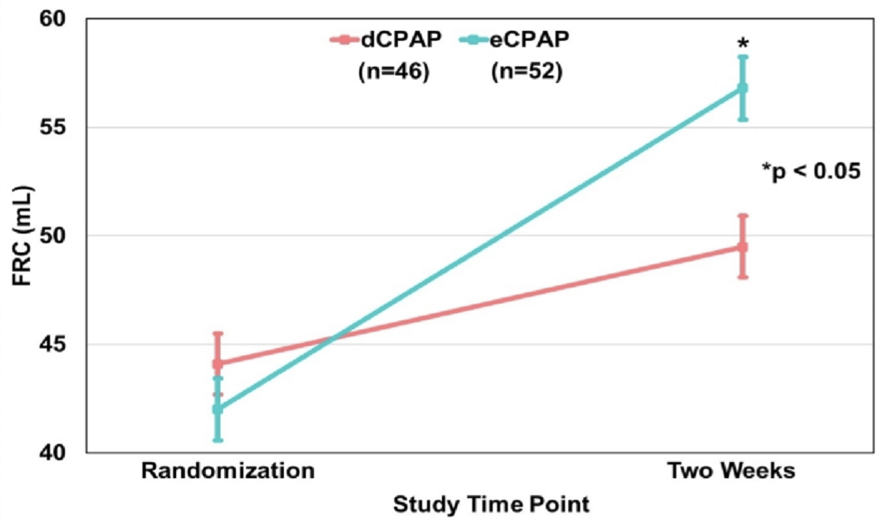
Finally, in the first session in the morning there was a trial of prolonged CPAP therapy, which disconcertingly had no zippy acronym. This should be illegal, how can a poor blogger think up catchy titles for their posts? Babies of 24 to 32 weeks GA at birth who were on CPAP, who were thought to be ready to stop their CPAP and who met stability criteria, had FRC measurements and were then randomized to have 2 extra weeks of CPAP at 5 cmH2O, using a bubble system.
The lungs grew more on CPAP. As you can see, after the extra 2 weeks the FRC was close to 20% greater in the prolonged CPAP group. At 6 months of corrected age lung volume was again measured, with a different technique which gives alveolar volume, and they also measured the diffusion capacity for CO,
At 6 months the prolonged CPAP treated lungs has a higher alveolar volume, and had better gas exchange.
I think this is potentially a major advance in respiratory care, it may be that babies who are at high risk of long term respiratory problems might be helped just by leaving them on CPAP for two weeks. Of course we don’t know if they had better or worse small airways function, or any difference in any clinical outcomes. But, many of us have major concerns about the very long term outcome of our patients, who may have deteriorating lung function later in life if they start out with fewer alveoli. This is potentially a big advance, if we can show that it is safe and has medium term advantages.
On my way to the PAS annual meeting in Toronto, I decided to spend a couple of days at Point Pelee national park. It is the southern-most point of Canada, a peninsula jutting out into lake Erie that is a landing spot for birds migrating north in the spring. It was, fairly recently, proven that most Warblers migrate at night, so after a long night flying across the great lakes many of them land at Point Pelee to “refuel” before heading onward to the Boreal Forest. Some very pretty birds can be found there, and some rarities.
When I parked my car I immediately saw a group of enthusiasts watching a little brown bird, which turned out to be a Harris’s sparrow; it was the first time this bird had ever been seen in the Park.
Red-headed woodpeckers are one of my favourite Canadian birds, this was only the second time I had seen them.
Green Herons are fairly uncommon in the Park
Loggerhead Shrike don’t usually come this far north, I think this was a first for the Park also
One of the prettiest birds you could see is the Prothonatory Warbler (apparently named after the vestments of an official in the Catholic church!)
If you are interested, there are other photos on my other blog at keithbarrington.com
I have been increasingly using video laryngoscopy in my practice, both when I myself perform the intubation, and when I am supervising a resident or other trainee. I usually ask them to use a VL when it is a nurse practitioner or RT that is about to intubate also.
It already seemed to me that the evidence was very supportive, with lower failure rates with VL than standard laryngoscopes, and I really appreciate the ability to see what someone else is doing when training them. A recent large RCT in adults with over 8000 procedures showed that the failure of the first intubation attempt was about 7.6% with direct laryngoscopy and only 1.7% with a video device. Intubation failure (needing more than 3 attempts or switching to a different device) was 4% with standard technique, and only 0.26% with the video. Ruetzler K, et al. Video Laryngoscopy vs Direct Laryngoscopy for Endotracheal Intubation in the Operating Room: A Cluster Randomized Clinical Trial. JAMA. 2024;331(15):1279-86.
I wish we could have success rates that high; multiple intubation attempts lead to local trauma, pain, increased physiologic deterioration including spikes in intracranial pressure and are associated with increased IVH. In marked contrast to the above study in adults, a recent single centre randomised study of video versus direct laryngoscopy for nasotracheal intubation in the newborn (n=89) had desperately poor rates of intubation on the first attempt: 49% success on the first attempt with the video, and 44% with direct laryngoscopy. Tippmann S, et al. Video versus direct laryngoscopy to improve the success rate of nasotracheal intubations in the neonatal intensive care setting: a randomised controlled trial. BMJ Paediatr Open. 2023;7(1). Infants received fentanyl and midazolam, some of them received vecuronium “if intubation conditions were considered inadequate after analgesia and sedation”, I have no idea how you can determine this prior to laryngoscopy. Most of the intubation first attempts were by trainees (60%), and the babies were intubated either in the delivery room or the NICU, most were preterm. Although I said first intubation success was “desperately poor”, such results are similar to many other studies which also have very poor success on 1st attempt.
What can we do to improve these poor success rates? Well, in addition to the RCTs, there is an ongoing multicentre quality evaluation initiative Near4Neos that has shown that you are more likely to be successful if you use muscle relaxant, and if you use a VL. But overall, in those database studies, success of the first attempt was still very low. With muscle relaxant 56% 1st attempt success, vs 33% with sedation alone, and 58% with the VL, compared to 47% with direct laryngoscopy.
Which brings me to the new trial, presented in Toronto at the 2024 Pediatric Academic Societies meeting, and published the same day in the NEJM. Geraghty LE, et al. Video versus Direct Laryngoscopy for Urgent Intubation of Newborn Infants. N Engl J Med. 2024. This single-centre RCT from Colm O’Donnell’s unit in Dublin randomised just over 200 babies, in the DR or in the NICU, who required urgent intubation. It therefore included preterm and term infants, and babies in the NICU routinely received premedication, which included a muscle relaxant.
The results showed a dramatic difference.
The paediatric residents success rate went from 40% to 70%, neonatal fellows from 53 to 77%. There were very few performed by staff neonatologists, even though the slide from the presentation in Toronto shows Dr O’Donnell’s ear as he is intubating with a VL:
As you can see from the next figure the advantages applied to small and preterm babies as well as the overall group, in the DR and in the NICU.
The successful first attempts took about 10 seconds longer with the VL (60 vs 50 seconds), but that did not increase the number of babies with major desaturation or bradycardia.
Of note, some of my colleagues performed a fascinating trial among paediatric trainees, Michael Assaad and Ahmed Moussa are 2 of my colleagues in Sainte Justine, and Ewa Gizicki was one of our fellows, the other authors of this trial are colleagues from across Quebec. They randomized residents about to intubate a baby to a 10 minute training session (if there was time depending on baby’s condition, of course), which consisted either of a 10 minute video, or “Just In Time” training, which was a 30 second video accompanied by practice on a mannequin, supervised by a staff who used scripted feedback depending on the difficulties experienced. Gizicki E, et al. Just-in-time Neonatal Endotracheal Intubation Simulation Training: A Randomized Controlled Trial. J Pediatr. 2023:113576. First attempt success rate was improved in the JIT group 54% compared to 41%. Rethinking exactly how we train and supervise residents for this important skill has been a focus of my 2 colleagues for a while, this approach requires a lot of the staff supervising, but it seems to work.
I think the accumulation of evidence and this new RCT makes it clear that Video-Laryngoscopy should be considered the standard of care of neonatal endotracheal intubation. It has universally been shown to reduce failure of the 1st intubation attempt, and even though the 1st attempt may be slightly longer, the overall duration of laryngoscopy is much shorter as you are more likely to only do it once!
Optimal Endotracheal Intubation Procedures:
Ensure that the appropriate person is doing the procedure, someone who has been well-trained, with the use of simulation before practising on babies.
High risk intubations should only be performed by an individual with proven competence. Intubating a 500 gram infant is not the time for a junior resident to “have a try”.
If at all possible, the baby should be premedicated, using an analgesic with a rapid onset (not morphine), and a muscle relaxant with rapid onset and short duration of action.
Oxygen should be administered during the procedure, preferably by high-flow nasal cannulae.
Video-laryngoscopy should be used for all neonatal intubations, both in the DR and in the NICU (note to self, we need to get them available for the transport team also).
Senior supervision of trainees is essential, and is also facilitated by Video-Laryngoscopy.
Endotracheal intubation is the most traumatic procedure that we perform frequently in the NICU, multiple intubation attempts harm our babies, and we should do everything possible to reduce their number.