
The other trial is a much larger multicentre trial with clinical outcomes. (Alexander T, et al. Nutritional Support for Moderate-to-Late-Preterm Infants – A Randomized Trial. N Engl J Med. 2024;390(16):1493-504), the gestational ages only overlapped by 1 week with the criteria in the trial I discussed in the previous post; this trial included babies of 32 to 35 weeks and 6 days.
To reiterate, the PEPaNIC trial, and a subgroup analysis of the newborn group, mostly babies who needed surgery, showed that babies receiving early TPN had more nosocomial sepsis, longer assisted ventilation and longer PICU stays compared to the late TPN group, who delayed for 7 days.
The new trial has a multi-coloured summary :
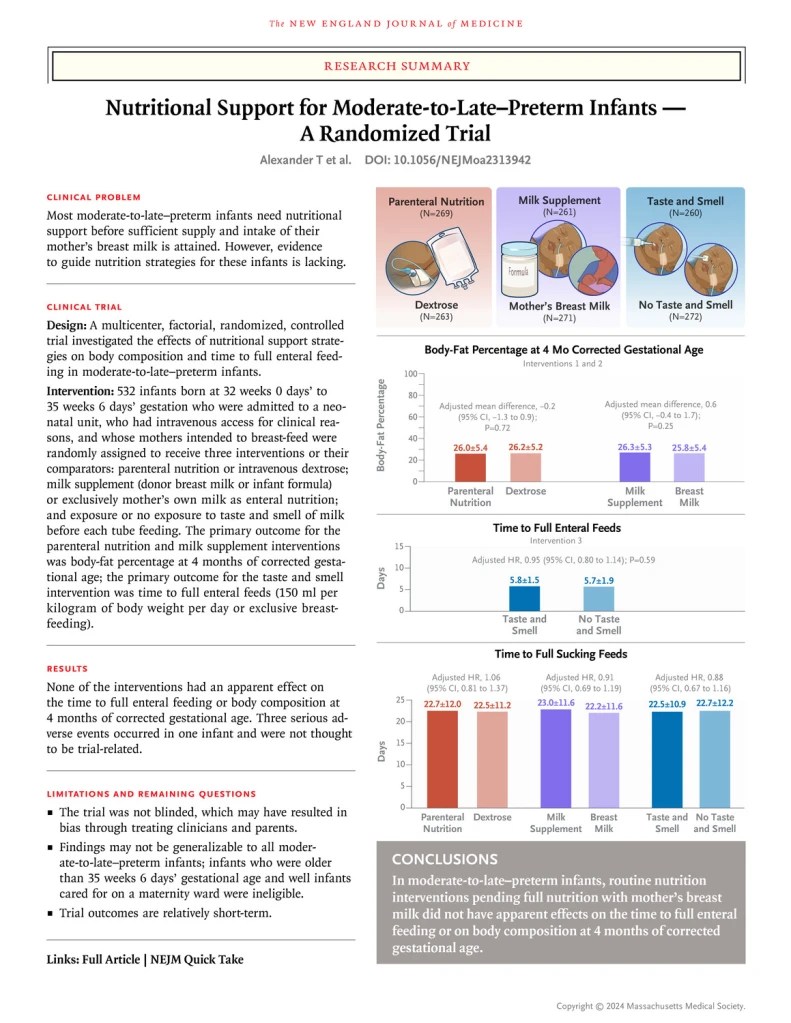
To be eligible for the study the baby had to be admitted to an NICU, have an IV access in place, and have a mother intending to breast feed. I will focus on the IV amino acid vs glucose solution arm of this complicated factorial trial, in which babies after randomization received either an amino acid solution or a glucose solution until they were full enterally fed. IV lipid was added, in either group, at the clinicians’ discretion, and the composition of the amino acid solution was according to local hospital practice. The actual intravenous protein intake averaged 1 g/kg/day over the first week, but, as many were stopped prior to 7 days of age, I can’t tell how much was being prescribed on the days while they were actually receiving the intervention.
The 269 babies in the TPN group over the 1st week of the study therefore received more total protein, averaging 2.6 g/kg/d, compared to 1.8 for the 263 babies in the glucose group. During week 2 the intakes were identical; almost all in both groups were off IV fluids. Fat intakes were also higher during the 1st week at 3.4 vs 2.8 g/kg/d, but carbohydrate intakes were a little lower at 8.6 vs 9.2 (2.8 vs 3.3 of which was intravenous). All of the enteral nutritional intakes were very similar between groups.
The time to full enteral feeds, and therefore discontinuing the TPN intervention, was a mean of 5.7 days in each group.
The primary outcome of the study was a measure of growth at 4 months of corrected age, that is fat-free mass. This outcome was identical between the groups at 4.9 kg.
There were 3 times as many episodes of culture-proven late onset sepsis with early TPN, and 3 times as many episodes of ‘probable sepsis’. Which sounds dramatic, but the actual number of each was 3 vs 1, and 3 vs 1, which, of course, is not statistically significant. Or, in other words, it might have been a chance difference, except that it is consistent with the other data which are accumulating. Other outcomes such as duration of hospitalisation were identical between groups, and most were not on respiratory support, so one cannot comment on duration of such support as an outcome.
In this low-risk group for serious adverse events, there was no sign of an advantage of receiving amino acid solution while enteral feeds were being established. There is a hint of adverse consequences.
Although the trials are not directly comparable, they have in common relatively mature newborn infants, and early versus delayed, or no, intravenous amino acid solutions.
They also have in common, as results, a difference in hospital acquired infections between groups. In the PEPaNIC results there are several different categories of infections, including airway infections which are notoriously difficult to define in newborn infants. So by extracting the culture-positive blood or CSF infections from the 3 trials, and putting them in a meta-analysis (I know this is questionable, but to give an indication rather than bullet-proof data) you get the following Forest Plot:
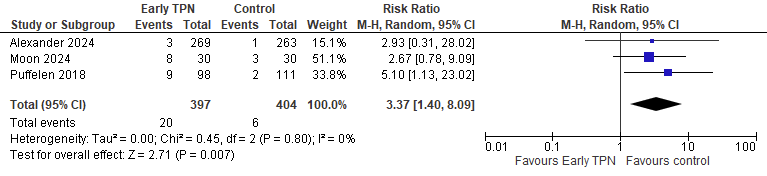
Alexander 2024 is the new publication of the DIAMOND trial, Moon i2024 s the trial I described in the last post, and Puffelen 2018 is the newborn subgroup of PEPaNIC.
Please note, this is not a formal systematic review or meta-analysis, just an idea of the similarity of the data between the trials, which have major differences. In particular, the babies in Alexander were a very low risk group, and more immature.
But, given the lack of any indication of benefit from early TPN in such babies, I think we must reconsider that approach. Waiting until the babies are clearly in need of parenteral nutrition, after several days, seems to be consistent with the available data. Early TPN is not indicated for babies at or near term, or for late preterm babies who are likely to be fed shortly. Exactly how long to wait, and what the indications are for TPN in such babies, will require more research.







Has anyone looked into nutritional support for very SGA term or late preterm babies? Is there any benefit in supplementing amino acids or TPN to those infants?
Pingback: Early Exclusive Enteral Nutrition: not Early, not Exclusive, some Parenteral, but interesting anyway. | Neonatal Research