
A new review article published in J Perinatol makes many claims about feeding patterns and NEC, but I think has seriously misinterpreted the literature (Assad M, et al. Dilemmas in establishing preterm enteral feeding: where do we start and how fast do we go? J Perinatol. 2023;43(9):1194-9). It is a little strange, that only 9 months ago a very similar publication, with a very similar title, appeared in the same journal, (Patel AL, Taylor SN. Dilemmas in initiation of very preterm infant enteral feeds-when, what, how? J Perinatol. 2023;43(1):108-13) and came to many different conclusions.
Trophic feeding
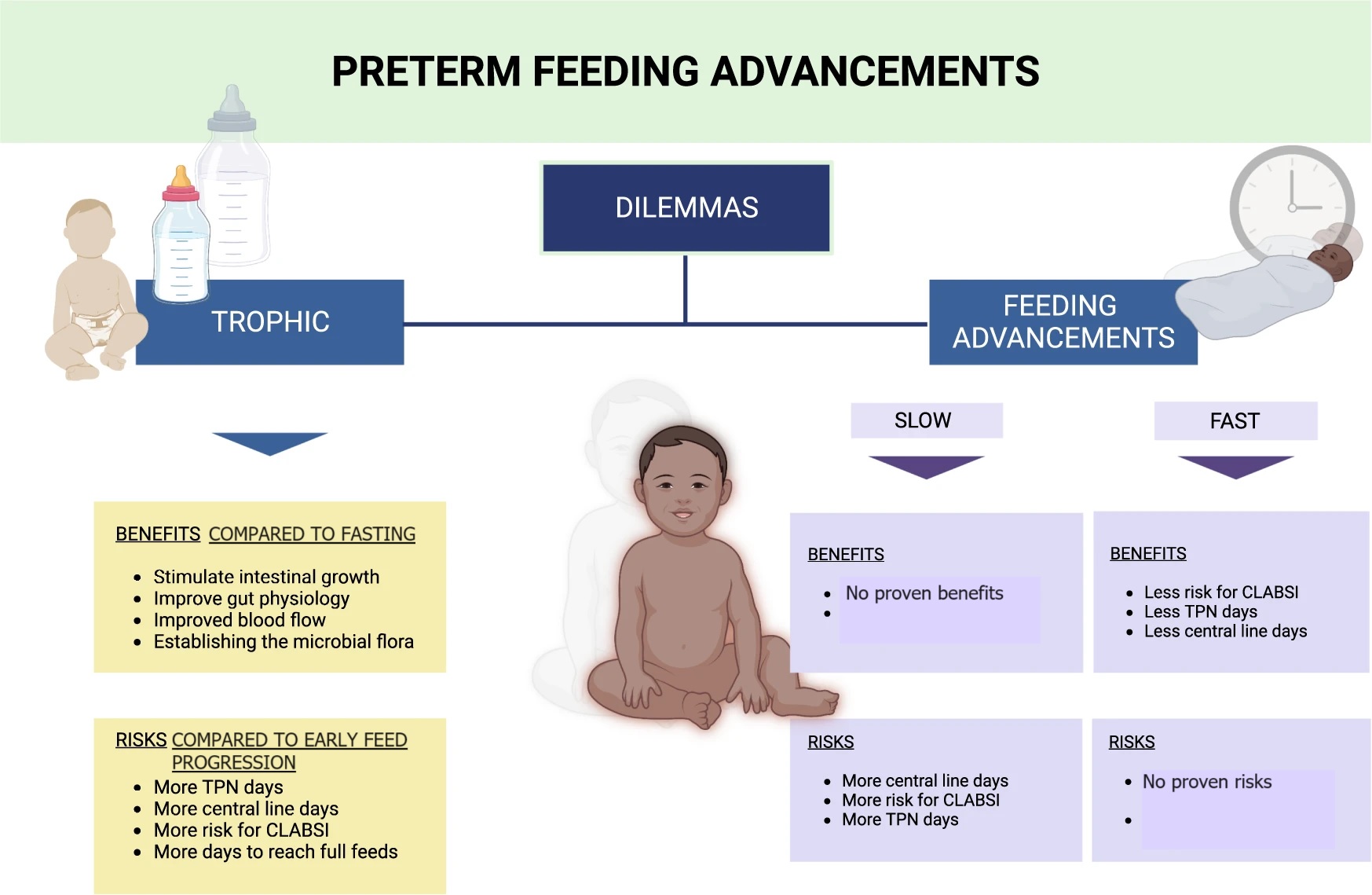
In the new article, the authors suggest that trophic feeding is advantageous, but that, of course, depends on what you compare it to. Trophic feedings are clearly preferable to a period of fasting, in terms of the physiologic responses, and do not increase (or decrease) NEC compared to a period of fasting. There is a Cochrane review, which dates from 2013, and showed no substantial benefit or risk of early trophic feeding, compared to a period of fasting: one further study, published since then, (Tewari et al 2018) also showed no adverse effect. In terms of limitations, few babies of high risk were included in those trials, and they tended to have very slow rates of feeding advancement once feeds were increased. Assad et al list the probable benefits of trophic feeding, but do not clarify that that is in comparison with a period of fasting.
Feeding patterns after a trophic period
Once you start to feed after a period of trophic feeding, the new review contrasts the study by Berseth 2003 to the trial of Salas 2018, suggesting that the results are not consistent. It is not surprising that the results were not consistent, however, as the trials were vastly different. The comparison made by Berseth was a period of trophic feeds, compared to immediate feeding advancement, among infants who had been starved for an average of 9 days after birth, and sometimes as long as 31 days! Indeed, the only study of different feeding patterns, or rates of advancement, that has ever shown an impact on NEC is that study by Berseth. Which means that if you are going to starve your babies for a week, then a period of trophic feeds is probably a good idea before increasing them. But most of us don’t do that anymore (or never did!).
The Salas study, in contrast, shows that among babies who were npo for 1 to 3 days after birth, immediate advancement, compared to 4 days of trophic feeding, did not lead to more clinical problems. There isn’t much other data comparing a period of trophic feeding to immediate progressive feeding increases.
Early feeding advancement
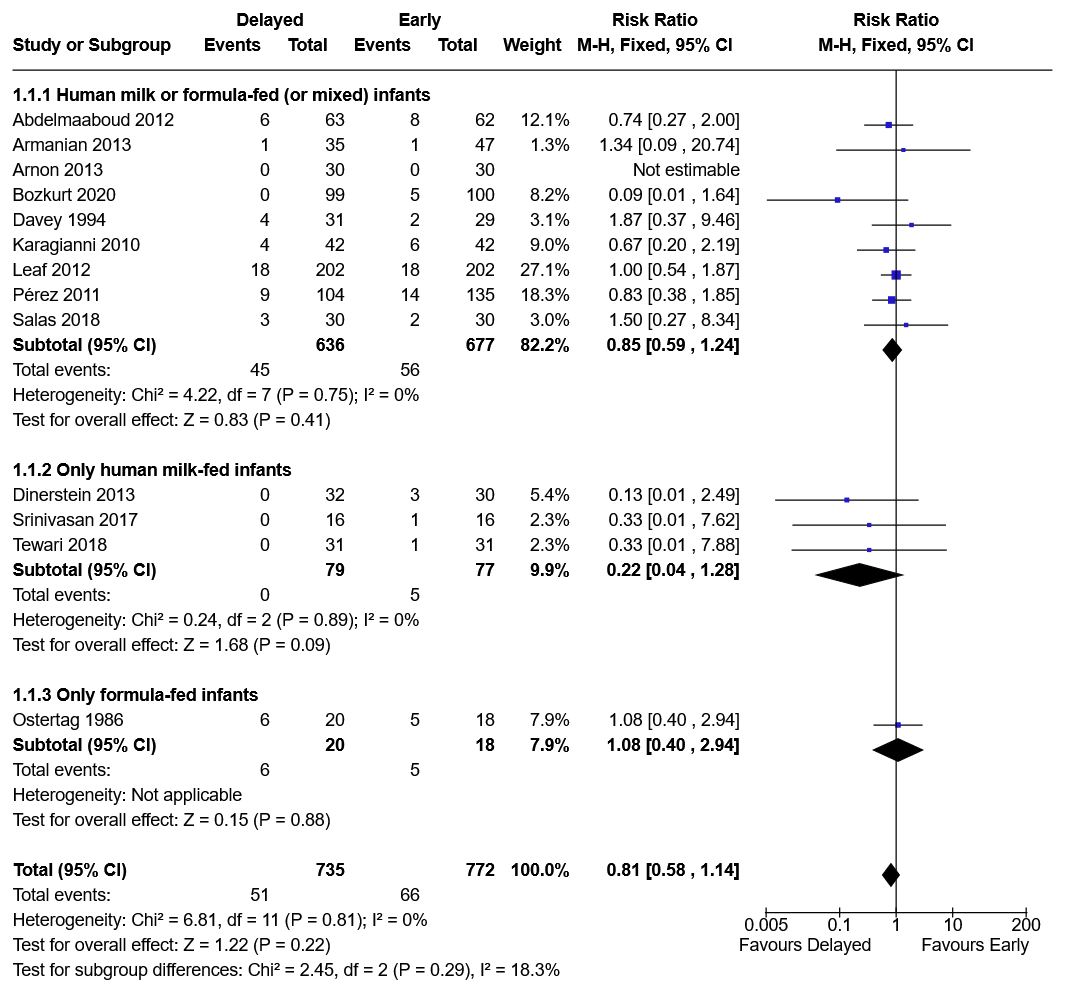
There are several trials that have investigated the impacts of starting feeds early, to starting them later, without a period of trophic feeds, in other words with an immediate start of feeding advancement. One of the best was limited to only very high risk babies, with SGA and abnormal antenatal dopplers. This was the ADEPT trial (Leaf 2012 in the figure below), which showed that the babies in either group had a lot of difficulty with feeding tolerance, but that there was no difference in outcomes of NEC, or survival, by group assignment (starting enteral feedings and immediate advancement at 2 days compared to at 6 days.) The Cochrane review showed no impact of delayed progressive feeds, compared to early progressive feeds, the Forest plot below is for the outcome stage 2 NEC, and shows that earlier feeding does NOT increase NEC.
Speed of feeding advancement
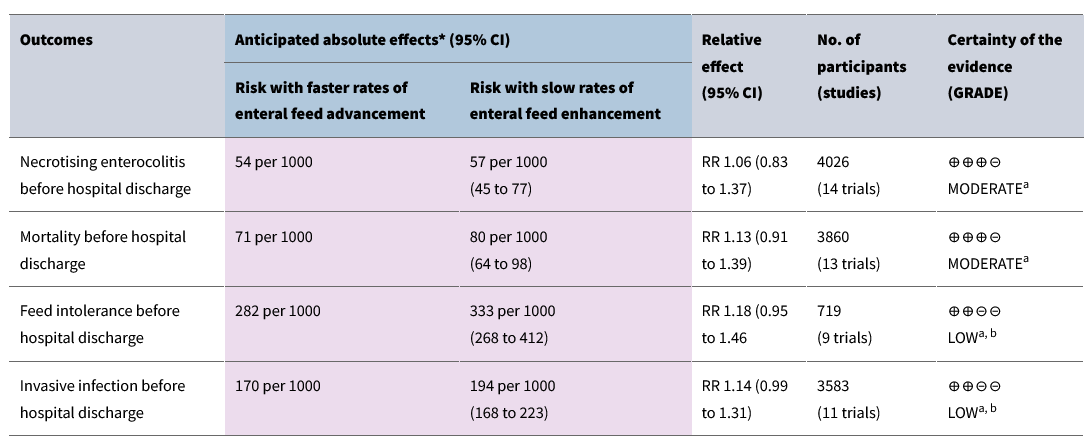
Once you start feeds, then the rate of increase has NO impact on NEC from any of the randomized trials. That is the other very misleading statement in this new review, the figure and the text suggest that slower feeding advancement leads to “possibly less risk for NEC” and “less risk for feeding intolerance”. Neither statement is supported by the literature.
The Cochrane review shows no hint of an increase in NEC with more rapid feeding advancement, the actual proportions with NEC are very slightly lower among those with more rapid feed increases. Similarly, there is no evidence that slower feeding advancement improves feeding tolerance. Feeding intolerance is, of course, a very difficult thing to quantify, but this is certainly consistent with my observations, some babies have regurgitations during the first few days of feeding, no matter how quickly you aim to advance the feeds. The comparisons in the various RCTs have usually compared a slower rate of feeding advancement to 30 mL/kg/day, occasionally as fast as 35 to 40 mL/kg/day.
This new review article sees to be based on personal preferences and inbuilt prejudice, with no evidence-base for many of the statements made. The following feeding plan is based on the conclusions of my review of the literature, and is very similar to the conclusions of an excellent published review from 4 years ago, (Kwok TC, Dorling J, Gale C. Early enteral feeding in preterm infants. Semin Perinatol. 2019;43(7):151159):
A feeding plan consistent with the best evidence
Some of the evidence is admittedly limited for some comparisons, especially in the very highest risk populations. Babies in shock or on inotrope/vasopressors could be an exception to the following plan, and they could be either kept fasting, or on low volume trophic feeds, but there really is no evidence to decide how to feed such babies, who may have reduced intestinal blood flow, and a limited capacity to increase flow after feeding.
There is no evidence that prolonged fasting, several days of trophic feeds, or slower advancement of feeds have any benefit in terms of NEC or feeding intolerance. Arriving at full feeds more slowly, however, does increase the duration of TPN, and all the associated complications, including late-onset sepsis (although, to be as stringently evidence-based as possible, the evidence for a reduction in LOS with more rapid advancement is uncertain).
Enteral feeding should be started on the first day of life, with maternal breast milk if at all possible. Feeds should immediately be advanced, by at least 30 mL/kg/day if tolerated, to between 160 and 200 mL/kg/day.
That’s it. Simple really! Give it a try.
In the new publication, there is a cute figure which summarizes the misinformation, and which I have, unfortunately, seen shared approvingly. With apologies to the authors, who I’m sure have the best intentions, I have corrected the figure to make it evidence-based.







OMG
I am glad I am not the author of this article! 😂
“Enteral feeding should be started on the first day of life, with maternal breast milk if at all possible. Feeds should immediately be advanced, by at least 30 mL/kg/day if tolerated, to between 160 and 200 mL/kg/day.” Is this statement true for babies born at less than equal to 26wk. Do we make a distinction between gestations especially for less than 25wk ?
There is very little actual published data to guide feeding practice in babies under 25, and especially under 24 weeks. The best centres have variable practices also, but, in general, they feed using the same approach as for more mature babies. That is, early starting feeds, and immediate progression according to tolerance. That is certainly our approach, we don’t make a distinction by GA, but start on day 1 if not on inotropes (most are not!) and advance as long as there is no regurgitation, even at 22 and 23 weeks GA.
Thank you for setting the record straight on this mess of disinformation that should have never been published in a respectable journal. In addition to all the flaws you pointed out, there is the fact that what we call NEC is probably a bunch of different conditions and not a single entity. Joe Neu has been making the case that we need to completely re-evaluate what this much over-diagnosed entity really is. Until we have an accurate diagnostic approach, we will continue to struggle to define the impact of feeding or other practices. That said, I fully endorse your early feeding and reasonably rapid advancement of feeds.
MK