
A long break since my last post. I have had a couple of trips, to Arizona and to Australia, and more recently to Washington DC. With each conference I now try, if I can, to take an extra few days to do some wildlife photography. You can see some of the results of the Arizona trip here, and the Australia trip here. Or head over to the home page of my personal blog and browse the many images that are now there.
I have also been busy doing quality control stuff in our NICU, and doing some weeks of clinical service, and additionally doing some writing. Indeed, writing has been my major role in these recent publications, writing early drafts and revising, and then re-revising after referee comments, which seem to be more “nit-picky” than before. I will probably write about these next 3 articles soon: Janvier A, et al. Fragility and resilience: parental and family perspectives on the impacts of extreme prematurity. Arch Dis Child Fetal Neonatal Ed. 2023:fetalneonatal-2022-325011. Thivierge E, et al. Guilt and regret experienced by parents of children born extremely preterm. J Pediatr. 2022. Girard-Bock C, et al. Gratitude, fragility and strength: Perspectives of adults born preterm about prematurity. Acta Paediatr. 2023. They are the result of 2 different projects, the first 2 from the Parent Voices Project and the 3rd from HAPI (Health of Adults who were Preterm Infants), both of which I am proud to have participated in. There is also another article in press, a review about the predictive value of early head ultrasound findings, with a former fellow as first author (Marie Chevallier) which will be in Seminars in Fetal and Neonatal Medicine, which I will certainly blog about.
The first of these recent publications that I will discuss here presents some of the data from the Parents’ Voices Project asking parents of extremely preterm infants in follow-up about their concerns. (Thivierge E, et al. Pulmonary important outcomes after extremely preterm birth: parental perspectives. Acta Paediatr. 2023) 44% of the nearly 300 respondents (all parents of extreme preterm infants) voiced concerns about pulmonary outcomes. Some of them related to the initial hospitalisation, and others about longer term respiratory difficulties. The concerns could be categorized as those related to how the babies were treated (such as, in the short term, duration of intubation and reintubations) and those reflecting the severity of the lung injury, such as needing oxygen at home, and the duration of oxygen treatment after 40 weeks PMA.
In the longer term there were also concerns relating to treatments received, such as the isolation of the family as they attempted to avoid infectious contacts, and indicators of lung injury, such as the impacts of increased respiratory distress (loss of sleep, need for respiratory medications). This table is a listing of the categories of concern that were developed from the answers to open-ended questions in a study conducted among parents of extremely preterm infants.

One thing that none of the parents mentioned was being in oxygen at 36 weeks, or a clinical diagnosis of bronchopulmonary dysplasia. Our focus on BPD, as diagnosed at 36 weeks, can therefore only be justified, in my view, if it is a good interim outcome, which strongly predicts long term respiratory pathology of interest to families. Unfortunately it does not do so.
As one example, the NICHD network evaluated the impact of different definitions of BPD, and compared them to two of the outcomes that the parents mentioned, pulmonary medication use and being rehospitalised for respiratory illnesses. (Ehrenkranz RA, et al. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics. 2005;116(6):1353-60).
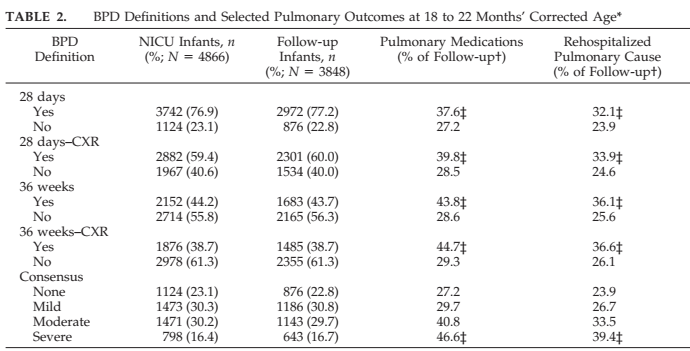
With the simpler dichotomous definitions, whether or not you include the requirement for Chest X-ray abnormalities, the positive predictive value for these outcomes is poor, as you can see it is around 40% for medication use, and 36% for rehospitalisation. The negative predictive value is also very poor, 30% of babies without a diagnosis of BPD nevertheless were receiving diuretics or bronchodilators, and 25% were readmitted to hospital for respiratory problems. The consensus NICHD definition doesn’t fare much better, many babies without BPD have those outcomes, and more than 50% with severe BPD do not.
Another very recent publication compared different BPD definitions at 36 weeks with long term outcomes, among babies from a single NICU in Amsterdam (Katz TA, et al. Comparison of New Bronchopulmonary Dysplasia Definitions on Long-Term Outcomes in Preterm Infants. J Pediatr. 2023;253:86-93 e4).. In this study an adverse respiratory outcome was “defined as occurrence of at least one the following: (1) ≥3 hospitalizations for respiratory and nonrespiratory reasons,24 (2) a visit to a respiratory specialist, (3) oxygen use at home between discharge and follow-up visits, and (4) chronic use of bronchodilators, antibiotics, or diuretics at 2 consecutive follow-up visits.”. These morbidities occurred in 22% of the babies at 2 years, and 18% at 5 years.
For any of the definitions they evaluated, the Area Under the Curve of the ROCs was not much better than chance.
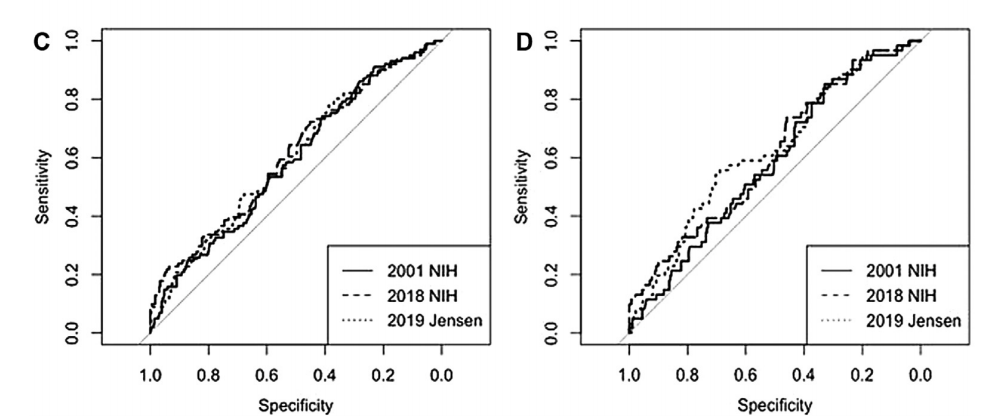
Graph “C” is the ROC for 2 year adverse respiratory outcome, and “D” for the 5 year outcome. The AUC (or C-statistic) were all between 0.55 and 0.58. Which is not much better than flipping a coin at 36 weeks! (AUC 0.5), and none of which were “statistically significant”. The ROC’s for Neurologic impairment or developmental delay were slightly better, but still mostly consistent with randomly predicting which baby would have difficulties.
I wonder what the best outcome would be for respiratory interventions in the preterm infant? In my mind the situation is similar to cerebral injury and neurodevelopmental outcomes, we don’t use head ultrasound findings as the primary outcome for brain protection studies, or for quality control. Although very imperfect, developmental evaluation at 2 years of age and neurological abnormalities at that age are what we use as the primary outcomes. Why not focus on respiratory outcomes during that same period as our primary measure of efficacy for respiratory interventions? These babies are all being followed anyway, so the additional cost would not be enormous, and most of the outcomes would be from parent questionnaire.
As an interim outcome, oxygen use at 40 weeks is a better predictor of serious long term morbidity than at 36 weeks, in the large CNN cohort study of Isayama T (Revisiting the Definition of Bronchopulmonary Dysplasia: Effect of Changing Panoply of Respiratory Support for Preterm Neonates. JAMA Pediatr. 2017;171(3):271-9), but in that study serious respiratory morbidity was quite serious! “(1) 3 or more rehospitalizations after NICU discharge owing to respiratory problems (infectious or noninfectious); (2) having a tracheostomy; (3) using respiratory monitoring or support devices at home such as an apnea monitor or pulse oximeter; and (4) being on home oxygen or continuous positive airway pressure at the time of assessment between 18 and 21 months corrected age”.
This outcome occurred in only 16% of infants on O2 or respiratory support at 40 weeks gestation, compared to 2% who were not on such support. In other words the PPV for that outcome was poor, but the NPV was very high. I would love to know what were the PPV and NPV for less extreme pulmonary morbidity. But at least oxygen at 40 weeks seems to be something that we could use as an interim outcome that parents actually care about: why do they care? I presume it is because it is a sign that the baby is staying in hospital because of their respiratory status, and their discharge is delayed as a result. It is quite uncommon in my NICU, and many others across Canada to send babies home on O2 before 40 weeks, they are usually at least at 42 weeks in my NICU before we organise home O2 if we discharge them with it.
Now that we have some sort of idea of the respiratory outcomes that matter to parents, we should try and find out how they prioritize them, and then try and construct an outcome variable that takes them into account, and that parents agree reflects the severity of their respiratory morbidity. Some recent papers have suggested that maybe we should do pulmonary function tests, which have the advantage of being relatively objective, but the major disadvantage of being somewhat invasive in young infants, relatively expensive, and not always correlating well with clinical impacts. I think a better idea of how respiratory morbidity affects the infant’s and family’s daily life would be preferable, and should be a priority for researchers in respiratory care of the preterm infant.







Has anyone examined predictive value for days of respiratory support adjusted for GA at birth?