
For another project I have been involved in, I reviewed a lot of studies addressing how and when preterm babies develop their feeding skills. Which I thought I would share.
Oral feeding is complicated! The first thing a baby has to do is to get milk from the breast into their mouth, this requires a lot more than suction. There needs to be a coordinated sequence of suction to keep the nipple in the mouth, and compression of the nipple by the tongue, coordinated movements of the palate and movement of the milk to the pharynx.
While doing my reviews I found the following video of an annotated ultrasound video of a baby breast feeding, I found this on the Medela web site, which doesn’t clearly attribute the source, however, it seems to come from the group in Perth WA, of Donna Geddes and Peter Hartmann, who published an article about the methodology and findings. Geddes DT, et al. Ultrasound imaging of infant swallowing during breast-feeding. Dysphagia. 2010;25(3):183-91.
You can see the tongue as the vaguely tongue-coloured block in the middle compressing the nipple, helpfully enhanced with the white milk ducts running through it, and the light blue coloured milk being ejected, and then moved to the back of the mouth into the pharynx. The nasal airway (in darker blue) is protected by the tongue being in contact with the palate, which then closes off the nasal airway as the milk bolus passes. It is easy to imagine the developmental maturity required for all of that to pass off without a hitch, and that is just the beginning, of course.
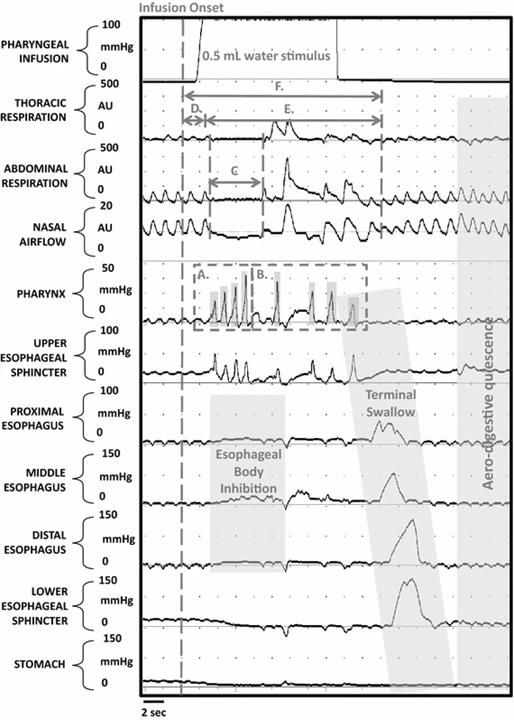
The subsequent stages include the initiation of swallowing and its co-ordination with a respiratory pause, and adequate oesophageal function. These steps require pharyngeal contractions to propel the milk posteriorly, relaxation of the upper oesophageal sphincter to allow passage and then oesophageal peristalsis, all of which have to be coordinated with respiration. In this study from Jadcherla’s group in Columbus OH, the coordination of suction and pharyngeal contraction was investigated, after the administration of a small liquid bolus into the pharynx, (Hasenstab KA, et al. Maturation Modulates Pharyngeal-Stimulus Provoked Pharyngeal and Respiratory Rhythms in Human Infants. Dysphagia. 2018;33(1):63-75)
If you follow the alphabet, A the initial pharyngeal response was multiple pharyngeal contractions, during which time (C) respiration paused, and oesophageal activity ceased, then the baby took a breath, and more pharyngeal contractions (B) propelled the liquid to the oesphagus, where a peristaltic wave can be seen descending, as respiration has re-started.
It isn’t surprising that this entire sequence is not mature in the fetus, who doesn’t need to breathe, or in the very preterm infant, who shouldn’t need to be breathing. In the same publication Hasenstab and others recorded 18 preterm infants (median GA 27 weeks) when they reached term, and again 4 weeks later.
The following figure illustrates the changes between the 2 recordings: the initial apnea was substantially longer at term, than later, and there were more peaks in the pharyngeal pressure, which were more variable.

In another study of 48 preterm infants at term equivalent age (Hasenstab KA, et al. Pharyngoesophageal and cardiorespiratory interactions: potential implications for premature infants at risk of clinically significant cardiorespiratory events. Am J Physiol Gastrointest Liver Physiol. 2019;316(2):G304-G12), half of whom were extreme preterm, heart rate decelerations occurred more frequently after a pharyngeal stimulus (0.1 to 0.5 mL of saline infused through a pharyngeal catheter) in the more immature infants, but most had a heart rate acceleration. Most of these studies have been performed during a bottle feed, as measuring pressures and flows is much easier than during breastfeeding! We have to assume that much of the physiology of the swallow, respiration, oesophageal activation, phase is the same. There are a couple of studies that have collected physiologic data during breast feeding, from the Perth Australia group, who have measured intra-oral pressures and performed simultaneous ultrasounds. They are responsible, I think, for the ultrasound image at the top of this post, and have published a cros-sectional study of preterms
Geddes DT, et al. Characterisation of sucking dynamics of breastfeeding preterm infants: a cross sectional study. BMC Pregnancy Childbirth. 2017;17(1):386. Th3 38 infants studied were of various gestational ages, but had all progressed to be feeding at the breast and where around 35 weeks PMA. Overall they showed that babies at this postnatal stage were able to generate a vacuum and had tongue movements similar to term babies, but they generated much less negative pressure (-40mmHg compared to the -115 that term babies generate). The preterms also had very variable sucking patterns, and also tended to have a progressive decrease in sucking vacuum during a feed, whereas term babies usually have a progressive increase. Indeed, as the nurses are often telling us, preterms do get tired during feeds! Full term babies have multiple sucking bursts, of more than 10 sucks, and few isolated sucks, here again the preterm babies were different, with fewer good bursts of <10 sucks, and more isolated single sucks. Of note, almost all of these babies/mothers were using nipple shields, which are of uncertain value, they may perhaps improve the efficiency of breast feeding, but might have an adverse effect on breast feeding duration.
Kerstin Nyqvist in Uppsala has studied a group of 15 extremely preterm infants, born between 26 and 31 weeks gestation, who had a history of either assisted ventilation (median duration 1 day) or CPAP, who were either in room air or on low flow oxygen. (Nyqvist K. Early attainment of breastfeeding competence in very preterm infants. Acta Paediatr. 2008;97(6):776-81) Most of the observations published were recorded by the mothers, after being taught what to observe:

You can see that the first signs of rooting occurred as early as 29 and a half weeks in one baby, but sometimes as late as 34 weeks, and more prolonged fixation and longer sucking bursts occurred progressively later. Also there was marked variability in the PMA at which certain activities were documented.
Can we help babies to develop these skills earlier?
It seems that use of a soother (pacifier or dummy) has benefits in the development of oral feeding skills. (Tolppola O, et al. Pacifier use and breastfeeding in term and preterm newborns-a systematic review and meta-analysis. Eur J Pediatr. 2022;181(9):3421-8), preterm babies randomized to pacifiers have shorter transition from gavage to breast feeding, by 3 days in the meta-analysis, and shorter hospitalisation (by 7 days!) They also found no evidence of adverse effects of pacifier use on breast feeding in full term babies.
An oral stimulation program was studied in a modestly sized masked randomized trial from Brazil, (da Rosa Pereira K, et al. Impact of a pre-feeding oral stimulation program on first feed attempt in preterm infants: Double-blind controlled clinical trial. PLoS One. 2020;15(9):e0237915) it isn’t entirely clear what the primary outcome variable was, but the program seemed to have advantages in the efficacy of the first oral feed (which seems to have routinely been from a bottle after 33 weeks PMA), and the transition to full oral feeding.
Another small (n=35) RCT from Marseille examined the use of a “uni-modal orofacial stimulation” technique, whereby the babies, 26 to 29 weeks GA, at <33 weeks PMA, had 12 minutes of stimulation of the cheeks, lips, gums and tongue by a gloved hand, followed by 3 minutes of non-nutritive sucking (presumably a soother), twice a day. Méziane S, et al. Cardio-Respiratory Events and Food Autonomy Responses to Early Uni-Modal Orofacial Stimulation in Very Premature Babies: A Randomized, Controlled Study. Children. 2021; 8(12). The primary outcome of the study was occurrence of apnoea and bradycardia episodes, but they also investigated the volume of milk taken during the first feed (presumably a bottle feed), which was 34mL compared to 29mL, and the subsequent feeds, which were not different between groups.
That study modelled their intervention on two studies from Fucile and others from Texas. (Fucile S, et al. Oral and non-oral sensorimotor interventions enhance oral feeding performance in preterm infants. Dev Med Child Neurol. 2011;53(9):829-35 and Fucile S, et al. Oral stimulation accelerates the transition from tube to oral feeding in preterm infants. J Pediatr. 2002;141(2):230-6). Both of these small RCTs seemed to show an accelerated transition from the start of bottle-feeding to full oral feeding with the stimulation program, which is this case was a 15 minute intervention once per day in the first study and twice a day in the later one. In both instances, the intervention started after the end of CPAP, and oral feeding commenced at an average of about 34.5 weeks PMA, and was determined by the clinical staff, not the researchers. Almost all of the feeds in these studies were bottle feeds, so we have no real idea if these interventions improve the progression of breast feeds.
As far as I can tell, from this review, promoting successful breast feeding in extremely preterm infants should include introduction to the breast starting early during skin to skin care, that the infants will start to show an interest, and preliminary rooting at between 30 and 32 weeks, and they may initiate single sucks soon thereafter. Whether there is any intervention that can improve the success rate of breast feeding, and can lead to earlier fully established breastfeeding, with potentially earlier discharge and fewer long-term feeding problems, remains to be clearly shown.
As the parental voices project has shown, feeding problems are one of the major concerns or parents of preterm infants (Jaworski M, et al. Parental perspective on important health outcomes of extremely preterm infants. Arch Dis Child Fetal Neonatal Ed. 2022;107(5):495-500), but such outcomes have rarely been reported in the literature.







Milk ejection plays its role during milk intake and swallowing without sucking happens very early in utero.
Thanks Keith. What is your view and practice on working on oral skills in these preterm infants while they are on non-invasive respiratory support (CPAP or HFNC)?
You might find these toolkits interesting – positive oral touch is point 6 (discussed in the second toolkit document): https://www.bapm.org/pages/196-maternal-breast-milk-toolkit