
There are a few trials on-going, or near completion or, as this one, just published, that should give us insight into what to do about an open ductus in the very preterm. This trial has major limitations, but does give us some information. Hundscheid T, et al. Expectant Management or Early Ibuprofen for Patent Ductus Arteriosus. N Engl J Med. 2022.
Babies of under 28 weeks gestation were randomized at 24 to 72 hours of age if an echocardiogram showed a PDA of over 1.5 mm diameter, and a majority left to right shunt. They either had expectant management (no pharmacological or surgical PDA closure, which was followed by all except 1 of the 136 in this group) or a course of ibuprofen, followed by a second, and then possibly a third and fourth courses, with an option for ligation under limited circumstances, n=137 in the intervention group.

My first question is whether infants in the PDA closure group were more likely to survive or not, and I don’t know! There is nowhere I can find in the document or supplemental material the mortality before discharge in the 2 groups. The intervention group had much higher mortality before 28 days, 18% vs 9.6%, and somewhat higher at 36 weeks, 18% vs 14%, but death before discharge (which is listed as an outcome in the supplement) is nowhere reported.
I don’t know about you, but I can’t interpret, or care very much, about any of the other outcomes if I don’t even know if survival is different.
It looks like there was about the same NEC in the 2 groups, and more moderate to severe BPD in the intervention group, so there was more of the composite outcome “death prior to 36 weeks, or mod/severe BPD or NEC (stage 2 or 3)” in the ibuprofen group, 64% vs 46%.
There are a couple of other issues that are not clearly addressed in the publication, a substantial proportion of the babies received paracetamol (acetaminophen to the North Americans), 38 % of the ibuprofen group and 25% of the expectant group, but whether this was for analgesia or as therapy to close the PDA is not mentioned. There were also a lot of babies who received diuretics, over 40% in each group, but for what indication, at what time, and for how long isn’t clear.
The study was stopped before halfway, so it was drastically underpowered to answer the weird question of what ductal treatment with cox inhibitors does to outcomes up to 36 weeks. I say a weird question because it is one that I don’t really care about at all! Were the babies more or less likely to survive to go home if they were treated? Did they have worse pulmonary outcomes, i.e. home oxygen, or prolonged hospitalisation for pulmonary reasons, or poor feeding because of persistent respiratory distress?
For the outcome that was reported, expectant management was “not inferior” to intervention. In other words if you stop looking at the babies after 36 weeks PMA, then leaving the PDA alone is not worse than treating it, but you have to guess about what happens after 36 weeks.
IF there were few deaths between 36 weeks and discharge, then expectant management appears preferable, but the relevance of the parts of the primary outcome are questionable: at 36 weeks there were more intervention group babies who needed oxygen, but the median duration of oxygen therapy (40 vs 41 days) and of respiratory support (55 vs 56 days) were almost identical between the 2 groups. Why is there no report about outcomes that matter? How many went home on oxygen? Was hospitalisation prolonged in the group with more BPD? Were the same number of babies feeding orally when they were discharged? These are things which have impacts on families, far more than the diagnostic label of BPD, and none of them are mentioned in the publication. They have made many other rather strange choices in data presentation, for example, I know that one of the babies developed West syndrome (which was likely diagnosed after 36 weeks!), and, from the table of adverse effects, I know that one baby in each group had a wrist abscess, despite not knowing the survival!!
There is 2 year follow up planned, so hopefully we will eventually discover the survival rates in the 2 groups in the trial.
Another trial published this year had some similarities (Potsiurko S, et al. Randomized Noninferiority Trial of Expectant Management versus Early Treatment of Patent Ductus Arteriosus in Preterm Infants. Am J Perinatol. 2022). In a single centre trial from Lviv, Ukraine, VLBW infants of under 32 weeks gestation were randomized at less than 72 hours of age if their PDA diameter was over 1.5 mm. They received either attempted closure (with either rectal ibuprofen or intravenous acetaminophen, n=104, the choice of rectal ibu or IV acéta was apparently randomized), or expectant treatment, n=104. with 8 of the expectant group having “rescue” PDA treatment at about 7 days of age.
These were, on average more mature babies, with a lower incidence of BPD, and there were no important differences in either survival to discharge (about 80% in each group), or the need for oxygen at 36 weeks (28% with active treatment vs 22% with an expectant approach). The power of the trial for excluding even major differences in outcomes is, of course, limited, with this sample size.
Most importantly however, I think there has been a huge failure of peer review for this trial, which is written in some parts as, and stated in the title to be, a non-inferiority trial, but it is no such thing. It is a comparative trial that did not show a difference between the groups, that is NOT the same as showing non-inferiority!
The sample size calculation is very strange to start off with, it starts by assuming that there is an outcome difference in favour of expectant treatment (death or BPD of 35% compared to 55%), and then calculating for an alpha of 0.01 and a power of 90% that they would not show a difference of greater than 10% beyond this difference. Which gave them a very small sample size for a non-inferiority trial, of 84 per group.
That really isn’t what is meant by a non-inferiority trial! The point of a non-inferiority trial is to show that the two approaches are not very much different, and that the experimental arm is not worse than the usual care arm, by an acceptably small amount, with a certain confidence. So to calculate the sample size you should start with the assumption that the two treatments have about the same outcome, and then calculate how much worse the new treatment could be without exceeding your “acceptably small amount”. If you use the non-inferiority margin that these authors have claimed in the methods of 10%, and that the incidence of “death or BPD” with standard care is about 40%, then with an alpha of 0.05 and a power of 80% (which are much more conservative than the calculations these authors have used) the sample size required is 297 PER GROUP.
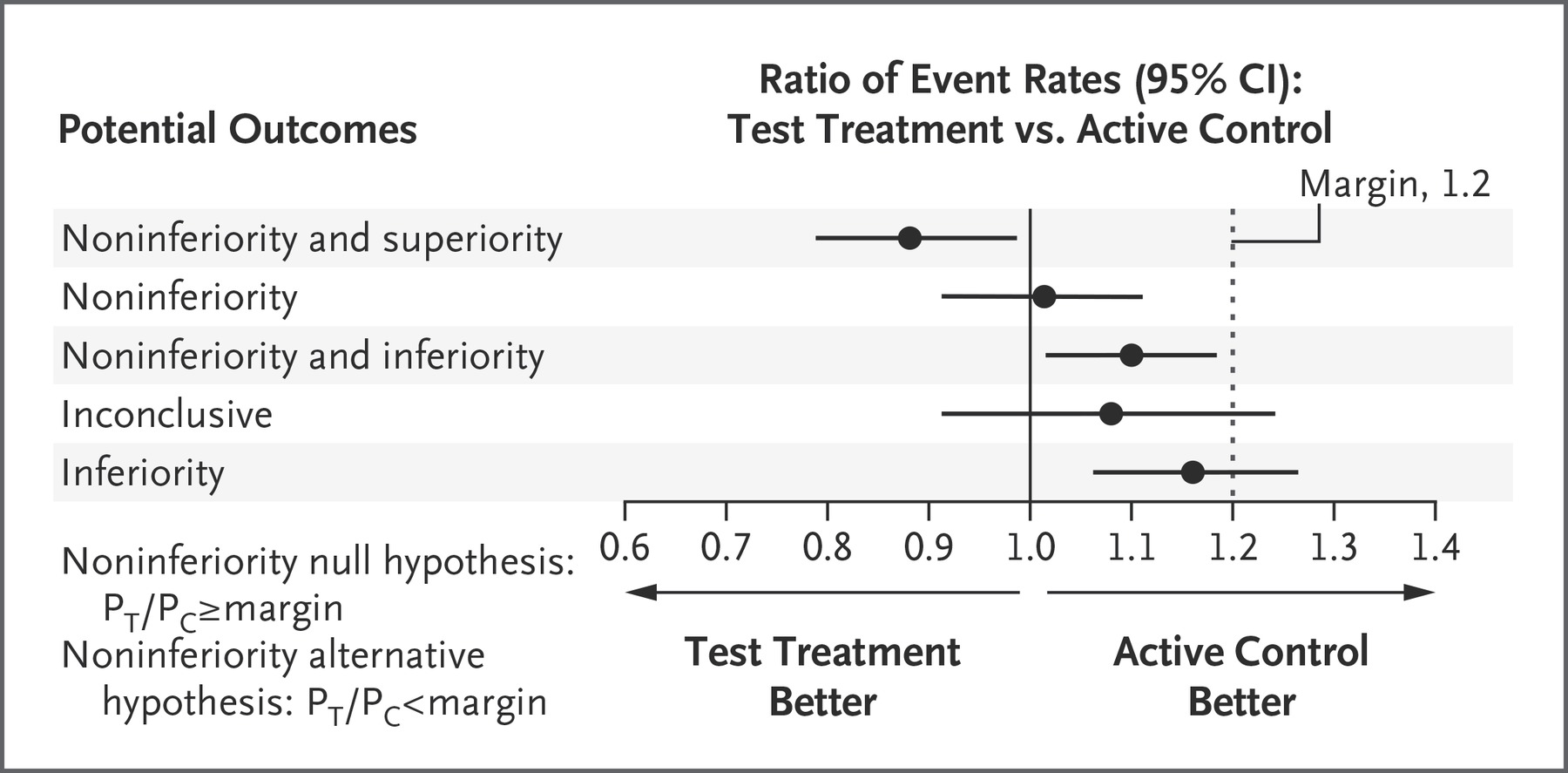
There is no mention in the results of the confidence interval of the difference between groups, which is essential to know if the non-inferiority margins were crossed or not. What I think they have actually shown is NOT non-inferiority, I have tried to visualize the results with the figure below, which shows the event difference between groups (death or BPD was 0.45 vs 0.39, or an event difference of 0.058, with 95% CI of -0.085 to 0.195, which overlaps both no difference and the non-inferiority margin of a 10% difference, and is therefore an inconclusive result.

You cannot say, based on this result, that expectant treatment is non-inferior to active PDA closure.
As a reminder, here are the possible outcomes of a non-inferiority trial, in a similar graphic form (from Mauri L, D’Agostino RB, Sr. Challenges in the Design and Interpretation of Noninferiority Trials. N Engl J Med. 2017;377(14):1357-67)
Another trial of early PDA treatment was published last year, (Roze JC, et al. Effect of Early Targeted Treatment of Ductus Arteriosus with Ibuprofen on Survival Without Cerebral Palsy at 2 Years in Infants with Extreme Prematurity: A Randomized Clinical Trial. J Pediatr. 2021;233:33-42 e2), this study randomized infants of under 28 weeks (minimum 24 wk) at 6 to 12 hours of age if they had a large PDA, which was calculated according to the postnatal age in hours (PNA), the minimum size to treat was 2.26-(0.078 x PNA)mm, so a 12 hour old baby with a PDA diameter >1.33 mm would be enrolled, or a 6 hour old with a diameter >1.8 mm.
A large proportion of the placebo babies received open-label ibuprofen after the initial course (62%, compared to 17% of the ibuprofen group), so the study is not very informative for other clinical outcomes, which really weren’t very much different between groups even though the PDA was more likely to be closed on day 3 and on day 14 in the ibuprofen group.
The primary outcome of this trial was the diagnosis of cerebral palsy at 2 years of corrected age. Survival to 2 years was a little more frequent in the placebo group, and CP was a little less frequent, but both differences could easily have been due to chance.
There are other trials of treating the PDA compared to a conservative approach, hopefully with designs which will inform us for the future which approach is preferable, based on clinically important effects such as survival to discharge and other outcomes which are of importance to babies and their families.







Pingback: Comment on my post about the Beneductus trial | Neonatal Research
Pingback: Closing the PDA… or leaving it alone? | Neonatal Research
Pingback: Is there any indication to close the PDA? | Neonatal Research
Pingback: Finally, a SMART approach for the PDA? | Neonatal Research