
My recent posts about resuscitation with an intact cord were rapidly followed by a publication of another multicentre randomized controlled trial, this time a cluster randomized crossover trial, of cord milking in babies who needed intervention. (Katheria AC, et al. Umbilical cord milking in non-vigorous infants: A cluster-randomized crossover trial. Am J Obstet Gynecol. 2022).
In this trial called “MINVI”, babies of 35 to 42 weeks GA were delivered vaginally or by cesarean, and evaluated during the first 15 seconds, prior to cord clamping. Those with pallor, poor tone, or apnoeic were then exposed to the intervention. If they were vigorous they had usual care (natural cord management).

Hospitals were randomized to one of two approaches, and, depending on the randomization, babies who qualified then had either early cord clamping (at the latest by 60 seconds) or had cord milking, which was performed with the cord intact, the cord being milked 4 times over a 2 second period each time, and milking about 20 cm of cord. The cord being clamped at a median of 29 seconds in the milking group (IQR 20s- 30s), compared to 20 seconds in the early clamping group (IQR 10s-20s). These durations are presumably estimates, as I don’t think there was someone assigned with a stopwatch to time the interventions (which is why the numbers are suspiciously round numbers!). Once half the study was completed, which took about a year, hospitals then were switched to the alternate approach (with a 2 month “washout” period).
The primary outcome of the trial was admission to the NICU for the following reasons: “respiratory distress (tachypnea, grunting, retractions), bradycardia or tachycardia, hypotonia, lethargy or difficult to arouse, hypertonia or irritability, poor feeding or emesis, hypoglycemia, oxygen desaturations or cyanosis, need for oxygen, apnea, seizures or seizure-like activity, hyperbilirubinemia, and/or temperature instability”. Admission just for observation or for antibiotics or because of low cord pH, for example, was not considered. There were numerous secondary outcomes, including principally HIE, and other outcomes that could reasonably be impacted by the intervention, such as jaundice and hemoglobin levels.
The cord milking group were less frequently admitted to the NICU for the above reasons, 23% vs 28%, however, after adjusting the analyses for centre, the confidence intervals of the adjusted Odds Ratio included no difference between groups, OR 0.69, 95% CI 0.41-1.14. Respiratory distress leading to NICU admission was less frequent with cord milking, other secondary outcomes are shown below

As you can see the cord milking babies were less likely to need respiratory support. There was also less moderate HIE, leading to less cooling, numbers of these neuro outcomes were small which is why there is no adjusted Odds Ratio.
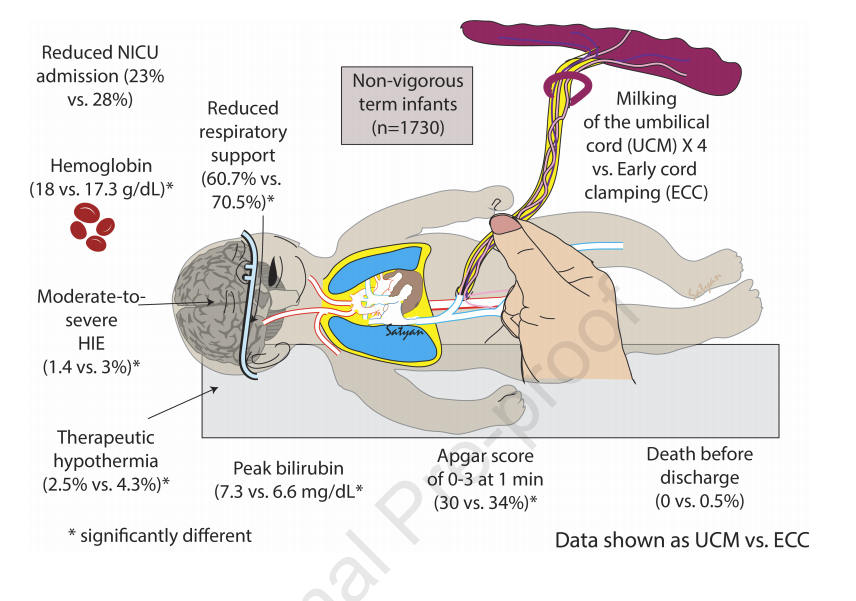
In the strictest sense this is a null study, with a primary outcome in the two groups being within the usually accepted limits of a possibly random effect. It certainly shows no adverse impact of the procedure, apart from the minor increase in bilirubin.
Anup Katheria, the principal investigator of this study, has previously published a review article (in 2018), which is open access, available via PubMed Central. He reviews the then available data, and the rationale which formed the basis for this study. I must say there is much less data from animal models regarding cord milking, and what is available is not reassuring, one study from Stuart Hooper’s lab, that I recently referred to, studied preterm lambs, (Blank DA, et al. Haemodynamic effects of umbilical cord milking in premature sheep during the neonatal transition. Arch Dis Child Fetal Neonatal Ed. 2018;103(6):F539-F46) and showed that if you did the procedure in one of the two ways they examined, they did not find much evidence that you actually increased blood volume. In that lamb study the milking was done in 2 different ways, the first was to release the cord between milks, so that it could refill from either end of the cord. The second method was to milk the cord, then keep it occluded near the lamb, so that it refilled from the placental end, then it was milked again. With the second method there was a net transfusion of about 9 mL/kg of blood. They also showed major haemodynamic fluctuations during the procedure, with blood pressure shooting up and down during milking.
You can see some of those impacts in this figure, of note there also was no net placental transfusion with physiological based cord clamping.
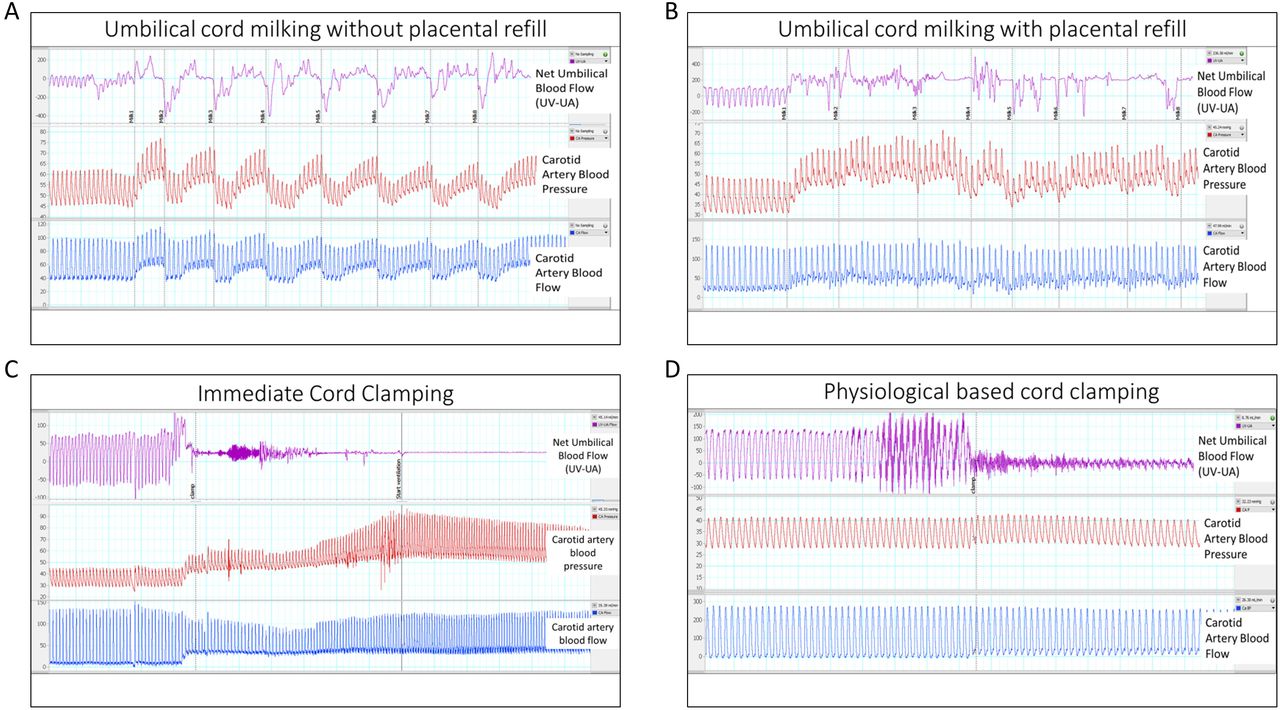
Although these impacts are concerning, the limitations of this lamb model are demonstrated by the lack of net placental transfusion with clamping after 3 minutes of positive pressure ventilation in the “physiological based clamping” group. Preterm babies with delayed clamping do have higher hematocrits and evidence that they receive a transfusion.
It isn’t clear to me whether the technique used in the MINVI trial is more reflective of the with or without placental refill group in the lamb trial, if I was doing it I think I would tend to hold the baby end of the cord closed with my fingers while the cord refilled from the placental end, (which is what Hooper’s group called WITH placental refill). It may be that the fluctuations in blood pressure and so on are less important in full term babies than they might be in the preterm.
What should be the response to these trials in the clinical realm? It might be too much to ask for a large RCT comparing clamping after PPV to cord milking in babies at or close to term who are non-vigorous at birth. In order to get an adequate sample size, an approach like MINVI, with cluster randomization and deferred/waived consent will be necessary I think.
That is probably the only way to resolve the conundrum, for now, based on these recent trials it looks like either approach would be acceptable, and both seem to be at least as good as early clamping, with no disadvantages of consequence, and all the differences being in favour of the alternative, physiology based clamping or cord milking. Personally, the physiology based clamping is something I find a more pleasing idea, in terms of the physiology, but it looks from MINVI that you can get the majority of the advantages, at least among term and late preterm infants who are non-vigorous.






