
I had to find a way of changing HeRO to Heroes as an excuse for posting a link to this video
But also the results of a long term follow up of the HeRO trial have been published. The original trial (Moorman JR, et al. Mortality reduction by heart rate characteristic monitoring in very low birth weight neonates: a randomized trial. J Pediatr. 2011;159(6):900-6 e1) was in babies of less than 1500 g. That trial found, of course, that babies who had their heart rate characteristics index displayed to the caregivers had a lower mortality than babies on the same monitors for whom the index was hidden. Further analysis of the data from that trial showed that mortality was lower only among those infants who actually had late-onset sepsis, and specifically within 30 days of a sepsis episode. Presumably, this is because sepsis episodes were detected sooner, and appropriate therapy started earlier. The improved survival after sepsis is illustrated in this figure
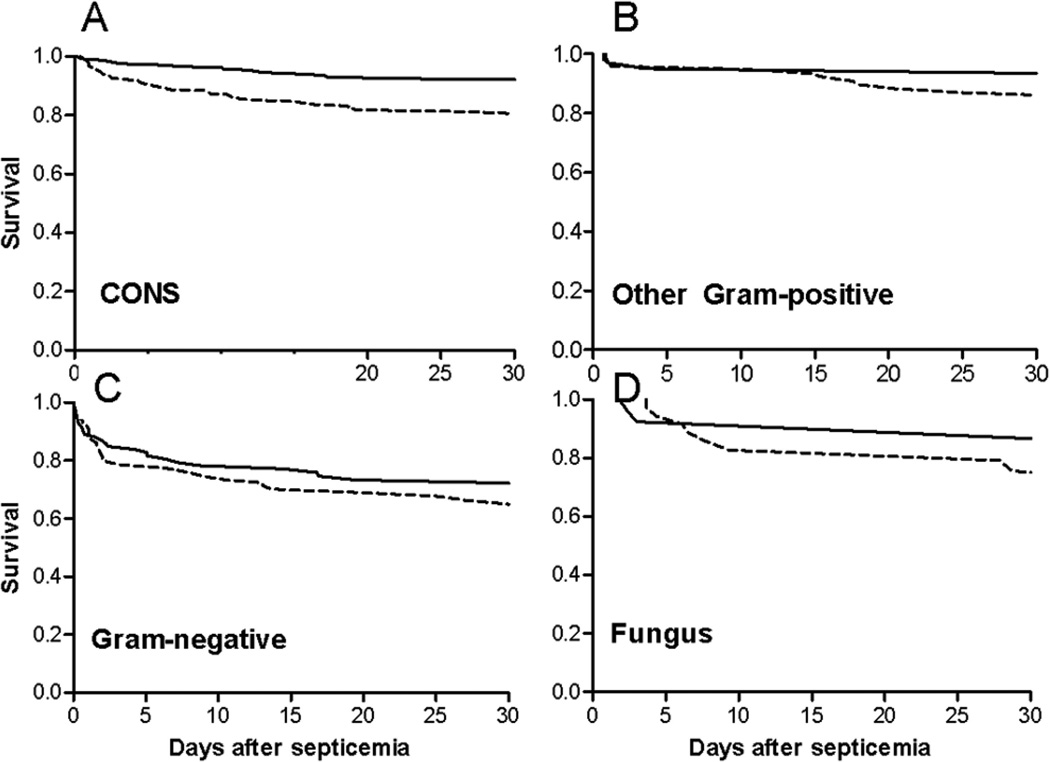
Organism-specific mortality based on heart rate characteristics (HRC) monitor display… Survival was higher in each organism group in infants with HRC displayed (solid line) compared with those with HRC not displayed (dashed line).
If that explanation of the results is true, you might also hope to find a reduction in long term adverse outcomes also. This new publication Schelonka RL, et al. Mortality and Neurodevelopmental Outcomes in the Heart Rate Characteristics Monitoring Randomized Controlled Trial. J Pediatr. 2020 investigated the developmental progress and neurological signs of a subgroup of the survivors, that is those with a birth weight under 1000g and born in one of the 3 hospitals who contributed the most to the enrolment. They were also centres with established expert follow-up. I want to repeat a comment I made on another recent post, the last of these babies was enrolled in May 2010, and therefore completed their Bayley version 3s and neuro exam at 18 to 22 months corrected age at the latest by July 2012. Why 7 years to publish these important data?
Survival in this subgroup of 638 infants was higher in the group with the HeRO score displayed, 76%, compared to 68% with the monitors hidden, relative risk of death 0.75 (95% compatibility limits 0.59-0.97).
Among surviving infants, the developmental and neurological evaluation showed the following:
| Neurological abnormality or developmental delay, survivors only | ||||
| Displayed | Hidden | RR (95% CI) | ||
| Overall proportion with at least one abnormality | 48/242 (19.8) | 37/206 (17.9) | 1.10 (0.75-1.63) | |
| GMFCS level 2-5 (moderate/severe CP) | 23/246 (9.4) | 13/210 (6.2) | 1.51 (0.78-2.9) | |
| Bilateral blindness | 4/247 (1.6) | 0/210 (0) | 0 (0-0) | |
| Deafness | 11/248 (4.4) | 1/210 (0.5) | 9.31 (1.21-71.55) | |
| Bayley cognitive <70 | 23/243 (9.5) | 15/207 (7.3) | 1.31 (0.70-2.43) | |
| Bayley language <70 | 36/241 (14.9) | 28/206 (13.6) | 1.01 (0.69-1.74) | |
As you can see there are not many differences between the 2 groups, and the small differences are all in favour of the control group. The exception being deafness which was surprisingly more frequent in the monitor displayed group.
Because there were more survivors in the monitored group you can express the data, if you wish, as ‘death or severe CP’ and ‘death or blindness’ and ‘death or a lowish cognitive score on the Bayley’, those results are highlighted in the abstract, but any regular readers of this blog will know my opinion about such composite outcomes. I think without trying to massage the data to find an outcome which is “statistically significantly” improved in the monitoring group, we can be reassured that there were more survivors in the monitored group and they had very similar outcomes to the controls. The authors of this study have done a lot of great work, on this project and many others, and I have a great deal of admiration for them, but I don’t understand why torturing the data to find a combination of outcomes that has a p-value less than 0.05 in favour of the HeRO system was thought to be so important. Improved survival with very similar long term outcomes is surely enough evidence on which to base decisions about an intervention, and in this case show that HeRO is the way to go.
As I also mentioned recently, I don’t think there is any intervention in neonatology that has increased survival and also worsened long term outcomes, and, most importantly, no intervention that increases survival but only of babies with a future quality of life that is worse than being dead. Surveillance of long-term outcomes in a trial such as the HeRO trial, and timely publication, is important for quality assurance and to ensure that we optimize interventions, and continue the enormous progress we have made in neonatology.
Before anyone comments that SUPPORT showed increased survival with worse retinopathy in the higher saturation group, that is true, but blindness was not different between groups, and the NeoProm group showed no adverse impact of higher saturations on any long term outcome despite better survival in the high saturation group.






