
This German multi-center trial randomized infants 400 to 1000 g birth weight to 2 different CO2 target ranges. The target ranges changed over the first few days of life:
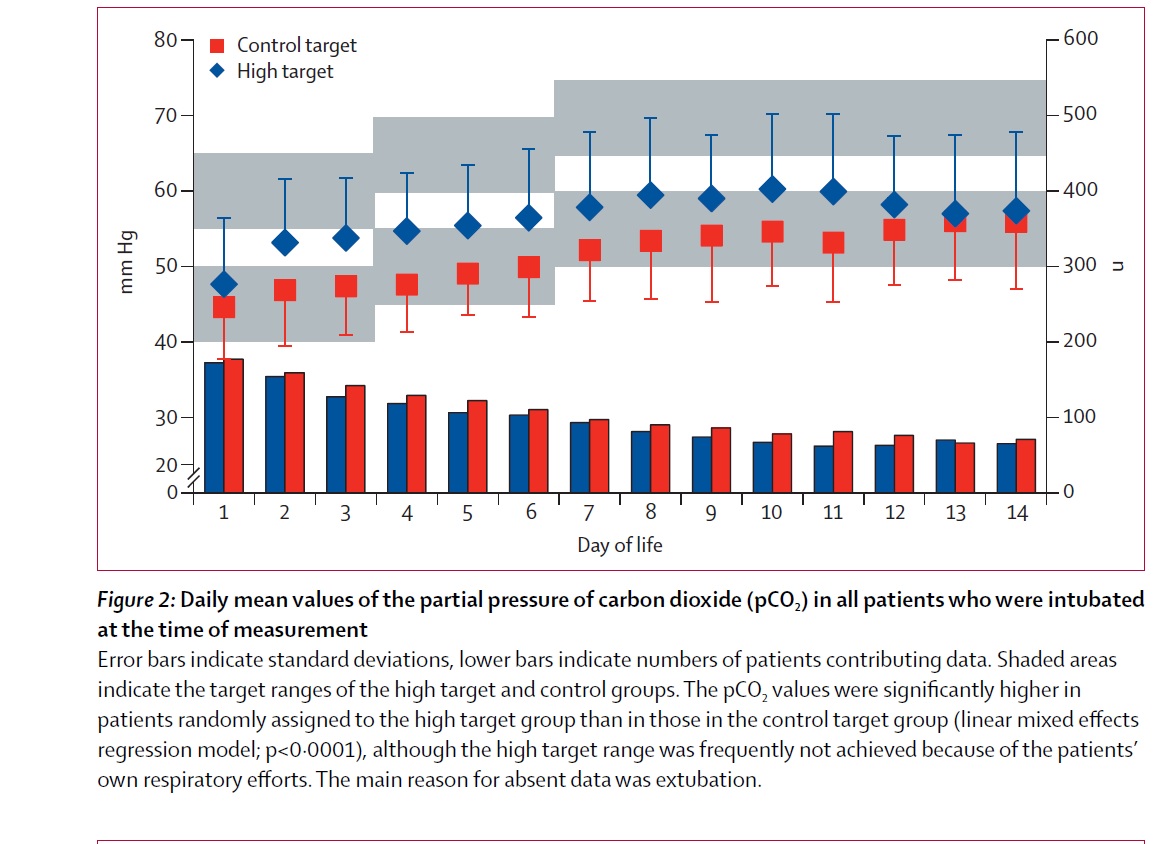
The high target group aimed at pCO2 values of 55–65 mm Hg on postnatal days 1–3, 60–70 mm Hg on days 4–6, and 65–75 mm Hg on days 7–14, and the control target at pCO2 40–50 mmHg on days 1–3, 45–55 mm Hg on days 4–6, and 50–60 mm Hg on days 7–14
The primary outcome variable was survival without BPD. Eligible infants were randomized within 12 hours of intubation and stayed in their group until 14 days of age.
This has been a difficult issue in neonatology, many have been reluctant to allow CO2 to rise in the first few days of life because of observations that infants with intraventricular hemorrhages had higher CO2’s. Prospective studies of allowing CO2 to rise however have not shown an increase in hemorrhage, so accidental or unintentional hypercarbia is a very different kettle of fish, denoting more severe events and so on. The idea of not increasing ventilation to normalize a CO2 is certainly an approach that I have taken for years, while acknowledging that there was no good evidence to say what the CO2 targets should be.
Two other related issues:
One, there is some evidence that respiratory acidosis may be protective in critical illness, so benefits of permissive hypercapnia might extend beyond less lung injury. Also attempting to buffer acidosis may well worsen lung injury. (Higgins BD, et al. Differential effects of buffered hypercapnia versus hypercapnic acidosis on shock and lung injury induced by systemic sepsis. Anesthesiology. 2009;111(6):1317-26. Laffey JG, et al. Buffering hypercapnic acidosis worsens acute lung injury. Am J Respir Crit Care Med. 2000;161:141-6)
Secondly, There are many ways to ventilate an infant. Just allowing a higher CO2 does not necessarily mean lung-protective ventilation. You can have a high CO2 with one very large tidal volume every 10 seconds, or with high frequency lower tidal volumes.
This study tried to address the second issue by favouring high ventilation rates (60 to 80 or greater initially) with inspiratory times between 0.25 and 0.35 s, and PEEP between 3 and 6. Initial peak inspiratory pressure was chosen to give ‘minimal to moderate’ chest rise. Once the peak inspiratory pressure was below 14 then ventilator rates could be decreased, and once below 30 inflations per minute the baby could be extubated.
There was an enormous use of bicarbonate. Which I find really strange, as I have not given bicarb to a preterm baby for over 20 years! Half of the babies in each group received at least one bicarbonate bolus. It was ‘allowed’ only if the base deficit was more than 8 mmol/L. They say that use of bicarbonate was “discouraged” which seems a weird choice of terminology when so many actually received it.
There was much less separation between the groups than the protocol would have suggested, (similar to an older trial by Carlo), they did mange to achieve more separation that that older trial.
The sample size was calculated based on a 20% relative reduction in the primary outcome variable (from 50% to 40%) with a power of 80% and a significance level of 5%, using a two-sided group sequential test with two interim analyses, required a maximum sample size of 830 patients.
And here is the big failure of this important study, it was stopped after “only” 312 infants had been enrolled. Because of slow enrollment the funding agency wanted an interim analysis,
The sequential design’s boundaries had not been exceeded at that time (ie, there were no detectable significant differences). The study design was changed from a three-stage group sequential design into a two-stage adaptive group sequential design with one interim analysis. The amendment was approved by the DSMB and the lead investigator’s responsible institutional review board. The interim analysis was based on 312 completed infants and carried out by an independent statistician. The results were presented to the DSMB, which recommended terminating enrolment. The funding agency’s review board concurred with this recommendation and it was implemented by the study coordinator.
The study showed no significant difference in the primary outcome between the groups, 36% in the high CO2 group, and 30% in the lower target group, Relative Risk is 1·21 (95% CI of 0·90–1·63). The 20% reduction in the adverse outcome that was hypothesized by the investigators seems unlikely given those results, but the early termination does lead to a great loss of an opportunity.
You can see here the grey areas, which represent the target CO2, and the coloured diamonds/squares the actual median CO2’s achieved.
What to make of this now?
Well, there are a number of reasons why this study may have shown no difference in outcomes between the groups; perhaps permissive hypercapnia as practiced like this is not protective of the lungs.
The authors screened over 1500 babies for inclusion, and over 400 were not enrolled because they weren’t intubated.
As you notice from that graph above, there was very little difference in the CO2 on the first day of life, which may be the most important period of life for initiating lung injury.
Perhaps the extensive use of bicarbonate infusions was an issue, if bicarbonate is as harmful to the lung as suggested by those experimental studies above, it may be that the use of bicarb in both groups eliminated any difference between groups.
Whatever the reasons, this study showed no clear adverse effect of permissive hypercapnia. So we have no better idea after this study what the optimal CO2 targets are for very preterm infants. The 2 ranges studied in this trial both seem to be within acceptable limits.
Perhaps we need to think about this differently, babies who are doing well, have a good response to surfactant and can be ventilated with ease may escape serious BPD even if the CO2 is kept within the lower of these 2 ranges. What we need to know I think, is when to increase ventilator settings to try and reduce CO2 and when we should let it go, allow the CO2 to rise rather than keep pushing ventilator pressures (or volumes, or amplitudes). I think there has to be a point when further increases in ventilation cause more damage than benefit. But where that is, and how to investigate it are rather difficult questions.
We will have to find other ways of protecting the lungs of our patients, and not just allowing the CO2 to rise. Minimizing lung injury in the first couple of hours of life, avoiding invasive ventilation, using volume ventilation, and getting babies successfully extubated are a few of the things that we need to investigate further.







This study just points out what a lousy outcome ‘death and/or CLD’ is.
The important outcomes are death, duration of respiratory support and neurodevelopmental status. No interim analysis should have been able to shut down such an important trial until these outcomes had been assessed. And to hear the premature stopping was prompted by the funding agency is unbelievable.