
Steroid metabolism in the very immature infant is… immature. Adrenal function is still developing in the fetus between 20 and 26 weeks, and a source of precursors from the placenta is important, but obviously disappears at delivery. Very preterm babies might have limited responses to stress, and therefore might benefit from administration of steroids. Some studies seem to show that extreme preterms who have lower cortisol levels, and/or lower responses to ACTH stimulation tests, have more mortality, or perhaps more BPD, but those data are confusing, and somewhat inconsistent. Babies exposed to chorioamnionitis have higher cortisol concentrations over the first week of life at least.
This micro-summary of the evidence underlying the rationale for replacement trials does suggest that some form of replacement is worth investigating, but for whom, and when?
There are a number of possible approaches to the very early use of hydrocortisone.
1) Immediate replacement therapy for all extreme preterm infants.
2) Immediate replacement therapy for selected infants
3) Slightly delayed (12 to 48H) therapy for selected infants with ongoing respiratory problems, or other diagnoses.
4) More delayed therapy (48h to 7 days) for selected infants with ongoing respiratory problems, perhaps with larger doses.
5) Therapy after 7 days of age, when lung inflammation has set in, with larger hydrocortisone doses.
A recent individual patient meta-analysis of studies which were referred to as “prophylactic” included 4 trials which, from this viewpoint, were in categories 1 and 3. (Shaffer ML, et al. Effect of Prophylaxis for Early Adrenal Insufficiency Using Low-Dose Hydrocortisone in Very Preterm Infants: An Individual Patient Data Meta-Analysis. The Journal of pediatrics. 2019;207:136-42 e5). I think that the implications of those 4 trials is quite different between group 1 (which is only the PREMILOC trial of 521 babies), and the other 3 trials which include 360 babies from Kristi Watterberg’s trial, and 100 total from 2 other trials, those three trials are in my category 3.
The PREMILOC trial (Baud O, et al. Effect of early low-dose hydrocortisone on survival without bronchopulmonary dysplasia in extremely preterm infants (PREMILOC): a double-blind, placebo-controlled, multicentre, randomised trial. The Lancet. 2016;387(10030):1827-36) did not have any postnatal illness criteria, but did exclude infants with severe growth restriction (<3%le), early rupture of membranes (<22wks). asphyxia (5-min Apgar <4) and congenital anomalies seen before birth. The growth restriction criteria would probably have eliminated more than 3% of babies from eligibility, depending on the definitions used. The other exclusions, probably fewer than that. The study did not include any babies of 23 or 22 weeks best-guess gestational age (BGGA).
Those other 3 trials included in this IPD meta-analysis are :
1. Watterberg, included infants of 500-999g if they were ventilated between 18h and 48h; they were randomized at an average age of 33 h. (Watterberg KL, et al. Prophylaxis of Early Adrenal Insufficiency to Prevent Bronchopulmonary Dysplasia: A Multicenter Trial. Pediatrics. 2004;114(6):1649-57). The 360 randomized infants received 1 mg/kg/d for 12 days, then 0.5 for 3 days, or placebo.
2. Peltoniemi 2005, who randomized 51 infants of 23 to 30 weeks and 500-1250 g birth weight, ventilated before 24 h (the larger babies were ventilated for >24h with O2). they received 2mg/kg/day for 2 days, then 1.5 for 2 days, then 0.75 for 6 days. (Peltoniemi O, et al. Pretreatment cortisol values may predict responses to hydrocortisone administration for the prevention of bronchopulmonary dysplasia in high-risk infants. The Journal of pediatrics. 2005;146(5):632-7). Hydrocortisone was started before 36 hours of age, but I can’t find the average postnatal age of administration.
3. Bonsante 2007, included 50 infants born at 24 to 30 weeks, and 500 to 1250 g, ventilated after surfactant, at less than 48h of life. They received 1 mg/kg/d for 9 d, then 0.5 for 3 days. (Bonsante F, et al. Early Low-Dose Hydrocortisone in Very Preterm Infants: A Randomized, Placebo-Controlled Trial. Neonatology. 2007;91:217-21). The actual age when the hydrocortisone was started is not clear.
Although I do think that including all of these trials in an IPD-SR is not unreasonable as a way of investigating the issues, it makes figuring out the implications for practice difficult; Premiloc asks the question: is it safe and effective to give all infants between 24 and 28 weeks BGGA low dose hydrocortisone within the first 24 hours of life? Will it likely improve outcomes without increasing hazards? Or more than the increase in hazards? The 3 trials in category 3 inform a response to a somewhat different question; is it safe and effective to give steroids to all infants of less than 28 weeks who remain intubated for respiratory problems at around about 24 hours of age?
If we divide the trials in this way we end up with much less power, and with results with wider confidence intervals as a result. The results of the PREMILOC trial must also be evaluated with reference to the much higher mortality in that trial than in my practice, or indeed in Canada overall. In PREMILOC the mortality for the combined group of 24 to 25 weeks gestation was 43% (almost identical between groups, 42% hydrocortisone and 44% control). In 2016 in the CNN report the mortality at 24 weeks was 27%, and at 25 weeks was 19%; 23% for the 2 GA weeks combined. (As a side issue, survival continues to increase, in the 2018 report mortality at 24 weeks is down to 22%, and at 25 weeks remains stable at 18%, for an overall of 20% mortality for the two weeks combined).
It is hard to know what to do with the results of a good quality trial like PREMILOC when the intervention group, who had better results after early universal postnatal hydrocortisone than the controls, have much worse results than our babies without routine hydrocortisone; indeed, double the mortality.
When the mortality is twice as high in the better group in a trial than our mortality without the intervention, can we expect any beneficial impact of the intervention on our outcomes? PREMILOC also showed a dramatically higher risk of late-onset sepsis with hydrocortisone than controls among the more immature group, 40% compared to 23%. It is also worth mentioning that 30% of the 24 and 25 weeks babies received hydrocortisone after the study period (slightly fewer in the hydrocortisone group than controls) and 11% of the HC babies and 13% of controls received post-study betamethasone, it isn’t stated how many received both.
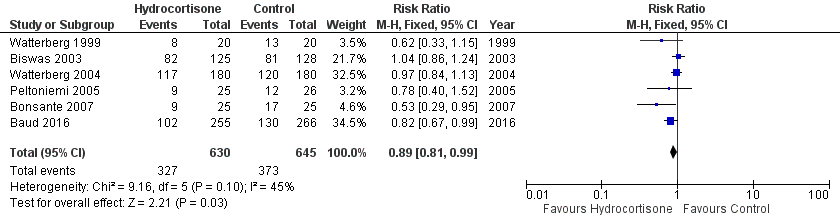
The results in the other trials also need to be taken in context, but as they are a selected subgroup of babies it is much harder to compare with local or national results. In Watterberg, for example, the mortality was 17% before discharge, and not different between groups. The original publication notes that the survival without BPD was basically identical between groups, 34% and 35%, or 43 and 42% using a physiologic definition. The IPD meta-analysis, in contrast, gives a slightly larger difference, and numbers which are different to either of the two reported numbers, 38% vs 41%. But in any case, if we put all the trials into a standard-type meta-analysis it looks like this, for the result of death or BPD:
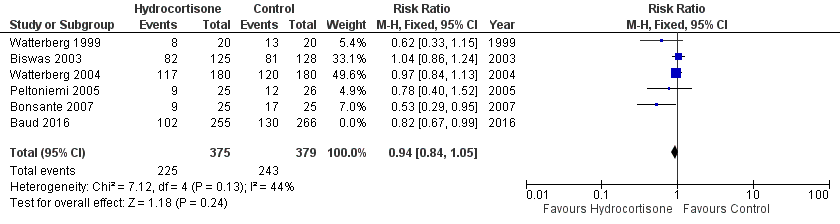
If we take out the group 1 trial (Baud) and just look at those with early selective treatment of babies being ventilated after the first few hours of life, it looks like this ;
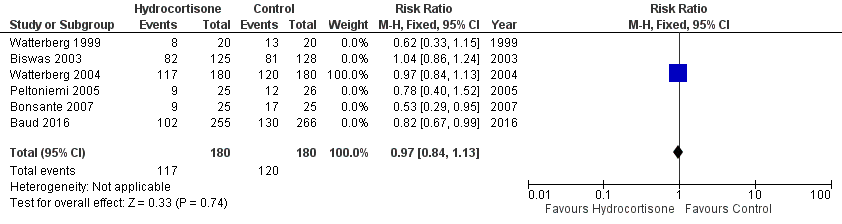
And if we take out the small trials, which are much more likely to show positive effects which are routinely exaggerated compared to larger trials, and take out the trial with co-intervention of hydrocortisone and T3 you are left with this:
There has been quite a lot of debate recently about systematic reviews and the fact that the Cochrane approach, of including all randomized babies, risks exaggerating the benefits of treatments, as smaller trials are much more likely to have positive results. Lower quality trials are also much more likely to have positive results.
I don’t like the idea of just eliminating smaller trials from the analyses, but sensitivity analyses focussed on larger trials, and on higher-quality trials, sometimes give different results to those obtained when all trials are included, and should be routine, I think, in a systematic review. Analyses could also be limited to trials which were registered prior to being performed, and further limited to trials where the primary outcome in the registration document is the same as the one in the final publication, to give an objective way of only including trials of high quality, even if they are small.
To return to the original question, what to do about postnatal steroids, I haven’t mentioned group 4 and 5 trials, but the Dutch multicenter trial of Wes Onland et al I discussed when it first came out, is in my group 5. It does seem to show a decrease in mortality with higher dose hydrocortisone after the end of the first week. There are some problems with extrapolatability for this trial also, I can’t find any published Dutch survival and BPD data more recent than 2011, but this article (de Kluiver E, et al. [Perinatal policy in cases of extreme prematurity; an investigation into the implementation of the guidelines]. Ned Tijdschr Geneeskd. 2013;157(38):A6362), after the change in Dutch guidelines to promote active treatment at 24 weeks gestation (thank you Google translate!), reported a 43% survival at 24 weeks, and 61% at 25 weeks, much lower than contemporary Canadian results, and 64% BPD incidence among survivors at 24 weeks, and 44% at 25 weeks. The Onland trial started in 2011, so these figures have some relevance. In the Flanders region of Belgium in 2011 (Draper ES, et al. Variability in Very Preterm Stillbirth and In-Hospital Mortality Across Europe. Pediatrics. 2017) survival at 24 and 25 weeks combined was only 40% and was 0 at 22 and 23 weeks.
For this trial, it is much harder to think about whether it may be relevant to my practice, the babies included were already receiving intensive care and had survived to a week of age, I don’t know whether the results of a similar group of babies in my current practice would be similar enough for me to be able to expect a similar impact on survival. But I am concerned that a mortality of 24% in the control group seems very high. If you use the online BPD calculator of the NICHD, using data from 2000 to 2004 (based on the publication by Matt Laughon), you can input data from a virtual baby similar to the average infant in the control group (male, 26 weeks, 710g, and 35% oxygen); the predicted mortality is 9.5%. substantially less than the mortality before discharge of the intervention group in Onland et al, which was 15.5%.
I know that comparing a point prediction from the online tool for a single baby similar to the mean baby in the Onland trial is not directly comparable to their findings, but it does give me pause to see so much higher mortality among the controls in the trial.
I think that I am not ready to give routine hydrocortisone to all babies between 24 and 28 weeks based on these data, nor to give them to 22 or 23 week BGGA babies. There are no clear data that giving them to babies at 24 hours of age who are still ventilated is beneficial either. I think, prior to changing practice and instituting a potentially hazardous treatment (increase in late-onset sepsis) I need a trial similar to Permiloc, which includes babies of under 24 weeks, in an environment with mortality more similar to current mortality in Canada, the USA, the UK, Germany, Australia and New Zealand, or Scandinavia (not an exclusive list!)
Perhaps a reasonable approach for the present would be to consider hydrocortisone therapy at 7 days of age if an individual baby’s predicted mortality is over say 24%. The Onland trial would suggest that this had a chance of reducing mortality, with little adverse consequence.







I absolutely agree with this analysis. The premiloc trial also included a large number of newborns who were intubated and mechanically ventilated (even at 26-28 weeks). That population in general does not seem to be representative of the Quebec’s practice and experience, with many of these babies >= 26 weeks being managed without intubation, on non-invasive support (in Quebec). The population of the study was intubated before study entry in about 80% for the kids 26-27 weeks, which sounds strikingly high for this « more mature » group. So in this group, if you would manage them without intubation, with CPAP/NIMV… would you get similar results?
The population in which I am very concerned about Death/BPD are those 22-25 weeks very immature newborns and the IUGR ones… and for them I cannot say that I can extrapolate any data from these studies. To use prophylaxis, with such a potent hormone, we should be careful and wait for more data that might provide increasing level of evidence. « Prophylactic » hydrocortisone may become the way to go, but it should be further investigated before implementation at large.
I think we should consider steroids way sooner in a shocked hypotensive infant as an early therapy rather than a rescue medication. I often also use them in prems with PPROM and suspected pulm hypoplasia.