
Imagine, if you will, that you work at a breast cancer center with moderately good results, but you have decided, as a group, to not offer therapy to women with stage 4- triple negative lesions. Survival is so low, you have decided, and the therapy so aggressive, that women should not be put through such a “futile” therapy.
But reports come in of other centers with survival well over 50%, long term outcomes which are excellent (as good as other types of breast cancer), and the short term complications of therapy which are similar to those of less aggressive cancer.
For the next woman who arrives in your center, what do you say? I think you would have 3 options:
1. “I know that in Superville they get good results, but they practice some sort of black magic: here in Ordinaryton we have decided that this is futile therapy so I am afraid you are going to have to die. We do have great palliative care though!”
2. “In Superville they are getting good results, so we are going to go ahead and do our thing too, let’s go!”
3. “In Superville they are better than us with other high-risk breast cancers also. We should gear up to offer therapy to women with triple negative cancers, let’s learn from Superville, and from the other centers who have also reported good results. Let’s make sure all of our team is up and ready. Let’s make sure we know how to do this the best we can. Let’s discuss each case individually with the patient, including all the details of the staging, and the risks of therapy and be ready to treat the next one who opts for intervention.”
It is fairly obvious what we should do to offer the best care (if transfer to Superville is not an option!) Just deciding that all such patients should die, while in several centers they can survive with a good quality of life, is not morally defensible.
Back to neonatology:
About a year ago I published a post talking about survival at 22 weeks gestation, a gestational age which is considered “pre-viable” by many practitioners, I noted that survival rates were high enough that “futility” could not be used as an argument against offering active support for such babies.
That post showed that several centers were achieving good survival at 22 weeks gestation. Total numbers of survivors were small, and very little follow up data was available.
The group in Iowa have just published detailed information regarding their outcomes, short and long term, over a 10 year period. Watkins PL, et al. Outcomes at 18 to 22 Months of Corrected Age for Infants Born at 22 to 25 Weeks of Gestation in a Center Practicing Active Management. J Pediatr. 2019. During that period active intervention was offerred whenever live birth at 22 weeks best-guess gestational age (BGGA), or more, was expected. The obstetricians offerred antenatal steroids and active surveillance. During that period there were 24 infants born alive at 22 weeks (I will concentrate on that subgroup, even though I know that intervention at 23 weeks is still not offered in many places. Some of the data are only available for the combined group of 22 and 23 weeks). Of those 24, 2 died before admission to the NICU, and 2 families opted for no resuscitation. None of the 22 week BGGA babies were delivered by Cesarean. This being from the USA, 7% of the mothers had no antenatal care prior to being admitted for threatened preterm delivery.
The obstetric team had time to give antenatal steroids to over 90% of the mothers, and half had more than 48 hours of coverage. Of the 20 babies admitted to the NICU, 14 survived to go home, and the list of in-hospital morbidities and their frequencies for the 22 and 23 week babies together are similar to what you would expect for extremely immature babies, and are not noticeably different from the 24 and 25 week cohort, that they also report.
Survival to discharge is remarkably good for the overall 22-23 weeks cohort, as well as for the 24-25 weeks group, 78% and 89% respectively.
With regard to long term outcomes at 18 to 24 months corrected age, the majority of infants evaluated had no or mild “NDI”. In this study the Bayley 3 test was done, and if the cognitive score was over 85, and the child was free of CP (or had a GMFCS of 1), hearing or visual impairment, that was considered no or mild impairment. 70 to 84 on the cognitive scale, or CP with a GMFCS of 2 or 3, was considered moderate impairment, and lower scores or worse CP was considered severe. 82% of the 22 week group were no, mild, or moderate, “NDI”, with 2 of the 11 evaluated survivors having severe NDI. The proportions between the different weeks of BGGA are similar, but do look a bit worse at 22 weeks, the numbers are small to evaluate statistically, however.
As you might realize if you have seen Annie Janvier’s recent contribution to John Lantos’ ethics rounds series in Pediatrics. (Janvier A, et al. Does It Matter if This Baby Is 22 or 23 Weeks? Pediatrics. 2019). We have offered active intervention to several babies at 22 weeks BGGA at our center, with a few hiccups during the hospital course of the first one, which you can read about in those rounds, but there has been a gradual acceptance in the NICU that survival and outcomes are good enough to offer NICU care.
Starting to do this, and getting good enough at it that you can get good survival (both numbers and quality), requires an integrated approach with Obstetrics. Offering NICU care if the obstetricians are not prepared to give steroids, is not a reasonable approach and will not likely be successful. No center is going to have many such babies, even in Iowa they only average 2 per year at 22 weeks, so having pre-existing protocols and a joint approach, all ready for the next mother who arrives is essential. If your obstetricians are reluctant to give steroids, you can show them this figure from (Travers CP, et al. Exposure to any antenatal corticosteroids and outcomes in preterm infants by gestational age: prospective cohort study. BMJ. 2017;356:j1039).
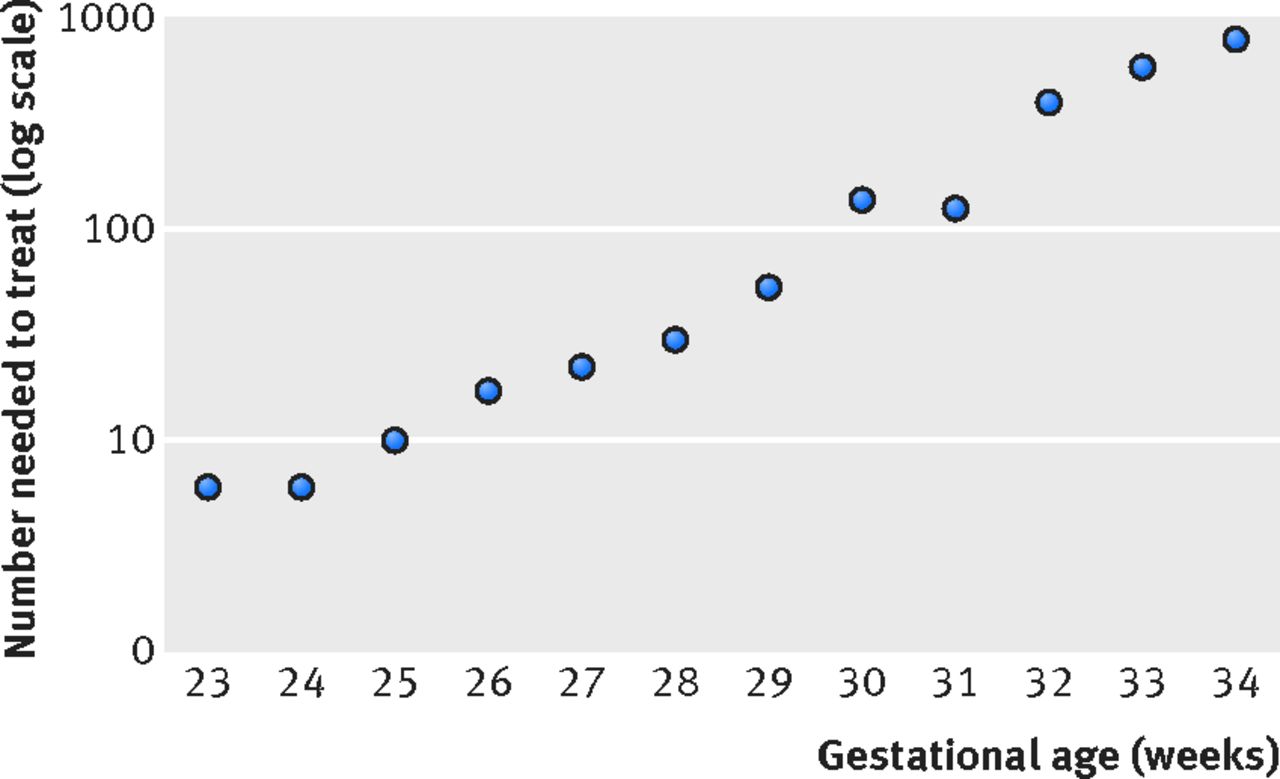
This is a graph of the number needed to treat per extra survivor, according to GA at birth. Data are from the Pediatrix data warehouse, and the total n is about 120,000.
At 23 weeks you only need to give 8 courses of steroids per extra survivor, compared to almost 1000 at 34 weeks! That study collected no data at 22 weeks gestation, but I can’t see any reason why the curve, which seems to flatten off a bit at the bottom, would suddenly leap upwards again.
In addition to the collaboration with obstetrics, consistency of the clinical approach, and a positive attitude seem to be essential. Having visited both Iowa and Uppsala recently, I can tell you that those 2 centers clinical approaches have multiple differences. Incubator care, ventilation, blood work, just about everything, seems different. The most important factor that they seem to have in common is that the people looking after the most immature babies believe in what they are doing, talk together frequently about how to improve their care, and expect that the large majority of the 22 and 23 week babies will survive. That has to include the entire team, from nurses to admission clerks to respiratory therapists (if you are lucky enough to be in a country with RTs), and of course integrating the parents.
I don’t think it is morally defensible to just tell parents ‘we don’t do that here’, and particularly not ‘it is futile’. Decision-making based on individual risk assessment, with a realistic option of high-quality committed active care should be offered.







So where do we work? In some kind of gray-zone-bourgade?
Have you seen the British Association of Perinatal Medicine new guidance on extreme prematurity? https://www.bapm.org/resources/80-draft-management-of-extreme-preterm-birth-before-27-weeks-of-gestation-2019 an excellent summary of existing evidence and making decisions based on multiple pieces of information rather than an arbitrary gestational cut off.
Probably time for ACOG/SMFM to update its latest guidance on this issue which says “Delivery before 23 weeks typically results in neonatal death irrespective of newborn resuscitation (5-6% survival) and, among rare survivors, significant morbidity is universal. (98-100%).”
http://www.acog.org/Resources-And-Publications/Obstetric-Care-Consensus-Series/Periviable-Birth
While from certain vantage points it may not be morally defensible to just tell parents ‘we don’t do that here’, or that ‘it is futile’, the processes and time it would take for hundreds of delivery centers in the US (or elsewhere) to accomplish similar results must be acknowledged. To unilaterally turn to individual risk assessment only of the patients (mother & fetus) and not the risks inherent in a center taking on anew the resuscitation and ICU care of these babies is myopic. The data published from Iowa are from a 10-year period, during which there would have been a realistic ‘learning curve’ and changes in practice. For a new center to attempt this would reasonably be expected to have a learning curve and attendant morbidity/mortality – the likes of which may well suggest to some physicians, nurses, or even parents that it may be “too risky, difficult, or fraught” to continue. Entire groups of neonatologists, nurses, hospitals, and OB/Gyns & MFMs will have to align values and purpose. While I agree that this new direction is a right, good, ethical direction to take, it must also be accompanied by disclosure in counseling parents of where the particular unit is on their path towards achieving outcomes similar to Iowa and that comparable outcomes cannot immediately be expected everywhere. As you know, resuscitation & care for the ‘fetal neonate’ is not the same as care for the neonate at 28 weeks or greater.
Thanks Brian, I agree with many of your points, and I don’t necessarily think that all babies born at 22 weeks should universally have active intensive care, on the other hand, I think that for average risk babies, or lower risk babies that an option to actively intervene with life-sustaining interventions should be available and that the argument that it is “futile” no longer holds.
I think we should always be transparent, and the parents of our first “22 weeker” were aware that she was our first. At that time there were no other centers outside of Montreal who were offering care, and she was too unstable, advanced, to transfer elsewhere anyway.
Improving care provision and preparing to provide such active care should certainly be done as an entire program. Despite our openness to intervene for some babies at such extremes, our outcomes are certainly not as good as Iowa, or Uppsala, or Kõln, for that matter.
Interestingly the recently published Canadian Neonatal Follow up Network report (which you can find a link to on this page http://www.canadianneonatalnetwork.org/portal/) shows that long term outcomes for babies born at 22 weeks gestation show that at 18 months the majority of survivors do not have significant impairment or developmental delay. Which is consistent with the Iowa data, and very much in contrast with the ACOG/SMFM statement mentioned by John Lantos,.
Thank you for this post, as the mother of a 22w2d boy I was very luck to be at a hospital where he was given the chance to survive, as they had a history of resuscitation and care for 22-23 week gestation neonates. Their experience in care for such a premature child lead to amazing outcomes.
This outlook is best for the doctors who refuse care to families or talk them out of care because they are not updated on current data and outlooks for these periviable neonates. When a practitioner’s practice/hospital does not/has not dealt with them before they fall back to old data and practices.
Sadly many a family is learning too late that a hospital down the street could have offered help and that they were given outdated advice to make decisions based on.
Thank you for the post, Keith, and to all for the comments. Our updated meta-analysis (Acta Paediatr. 2019 Jul;108(7):1237-1244. doi: 10.1111/apa.14693.) also again shows that children at 4-10 yrs of age who were born at 22-25 weeks have comparable rates of “severe” (by our labelling) neurodevelopmental ‘disability’.
There is also a poignant piece recently published in Pediatrics, providing ideas for how to support families in their decision making during this difficult and complex time of anticipated extremely preterm birth. It is worth a read (Pediatrics. 2019 Nov;144(5). pii: e20191625. doi: 10.1542/peds.2019-1625. Epub 2019 Oct 2.).
Thank you for this thoughtfully written and data driven article. In particular, I appreciate your analogy to stage 4 triple negative breast cancer. It puts the ethical issues at play into terms that an average adult can understand because so many people can find a way to relate to the breast cancer scenario.
My background is that I am a pediatric subspecialty surgeon who recently delivered a son at 22 weeks. My initial care started while on vacation at a hospital that was at least willing to consider active management of 22 weekers. Assuming this was standard at academic medical centers, when my condition stabilized I made my way home, only to find myself going into labor upon arrival at the airport. I went right to my local hospital expecting to receive the same level of care that had been discussed previously, only to have all of the things I asked about (tocolytics, magnesium, steroids) flat out denied by the MFM team because “they don’t work until 23 weeks.” My own OB even told me they “don’t make breathing tubes small enough” for my 500g child, which didn’t sound right since I could have sworn I’d been involved in the care of 400g babies in my own professional life, but I was simply in too fragile of a mental state to conjure up any specific examples.
In the subsequent weeks of my maternity/bereavement leave I spent much time exploring the literature on periviable births and was shocked at the verifiably false things I had been told. I deeply regret that I was in too diminished of a mental state to independently verify the information being given, but frankly a patient shouldn’t have to do that. This has been particularly difficult for me to process given that I delivered across the street from an exceptional children’s hospital where I happen to work. As a pediatric provider, it has long astounded me that aggressive and extraordinarily expensive medical care is so freely recommended late in life while it is often discouraged at the beginning of it. Never has that been more apparent to me than it is now that I find myself also in the shoes of a bereaved mother.
Carolyn, I am moved by your compelling and heartfelt message – coming from a tragic experience. We, collectively as health care professionals working in a country with a fractious health care system, will need to effect a number of changes – over a period of time that will require additional educational, philosophical and policy changes – in which the possibility of survival and good outcomes are acknowledged and allowed. Like other extremely premature gestations, 22 week EGA infants may not all survive, concurrent palliative care support may well be reasonable, and some babies may be discharged after lengthy hospitalizations, even surgery as you note, and some with chronic or debilitating conditions, though still loved by their families. Yet these considerations should of themselves disqualify them from a trial of life…effective resuscitation, NICU care, and good NICU Follow-up.
Brian, thank you for your remarks. The fractious healthcare system is indeed a challenge. Your comment above, “Entire groups of neonatologists, nurses, hospitals, and OB/Gyns & MFMs will have to align values and purpose,” is both right on the mark and a very difficult goal to achieve in such a system (as are many other team-based goals). In my own experience, the OB/MFM team behaved as if there was such a unified front, a black-and-white agreed upon hospital policy, and discouraged me from speaking with a neonatologist…”oh, I guess we could call them tomorrow, but they are just going to tell you the same thing I am, we won’t do anything unless you make it to 23 weeks.” In post-mortem discussion with a neonatologist friend-of-a-friend at that same hospital, it became apparent that no such inflexible policy exists. Moreover, I have become aware that a hospital literally half a mile down the road has not only attempted resuscitation at 22 weeks, but been successful at it.
I have to assume the fictitious policy purported and the lack of suggestion to transfer me is the result of the intrinsic biases and values of the individuals who were on call the night I presented. Since my own loss, I have had the opportunity to connect with numerous mothers in the US and Canada who have had very similar experiences, some even at 23 weeks. It is amazing how dated information and attitudes are so pervasive. In a healthcare environment where “shared decision making” is increasingly emphasized, this paternalistic approach must end.
There is no one answer to this (or any healthcare issue) that will be right for every patient who walks in the door. Some families will favor avoiding aggressive medical intervention while others will want to expend ever option possible. At the end of the day, families should be provided with thorough and accurate information so that they can make an educated decision that aligns with their own values, not be forced to conform against their wishes. I work with many families of seriously disabled children and you are correct that despite their challenges, those children are loved and enjoyed. That love is not something to be dismissed and the possibility of life with disability, or the possibility of failure, is not a good enough reason to refuse to try.
Pingback: The jaundiced eye of the beholder | Neonatal Research