
MOM is best, because it leads to the lowest incidence of NEC; but why? (if you didn’t read part 1, MOM is Mother’s Own Milk)
The impacts of milk processing which create the differences in milk composition, detailed in my previous post, may be the link to the increased incidence of NEC. That effect could be mediated by changes in the intestinal microbiome. There have been several recent publications about this:
Cai C, et al. Feeding practice influences gut microbiome composition in very low birth weight preterm infants and the association with oxidative stress: A prospective cohort study. Free Radic Biol Med. 2019;142:146-54.
Parra-Llorca A, et al. Preterm Gut Microbiome Depending on Feeding Type: Significance of Donor Human Milk. Front Microbiol. 2018;9:1376.
Ford SL, et al. Improved feeding tolerance and growth are linked to increased gut microbial community diversity in very-low-birth-weight infants fed mother’s own milk compared with donor breast milk. The American journal of clinical nutrition. 2019;109(4):1088-97.
Zanella A, et al. Influence of own mother’s milk and different proportions of formula on intestinal microbiota of very preterm newborns. PLoS One. 2019;14(5):e0217296.
These studies are relatively consistent, although the complexity of microbiome data and the ways in which they should be presented and analysed are still developing, and can be quite confusing to a non-specialist, like me. Overall, the fecal intestinal microbiome in MOM fed infants is more diverse, as shown by increases in alpha diversity; which are measures of how many different bacteria there are and how variable they are. Differences in beta-diversity, which are ways of comparing these diverse bacterial communities, have been found between formula, human milk and donor milk.
One very recent interesting study by Zanella et al reported 5 groups of babies, with exclusive MOM (LME in the figures), exclusive formula (FLE), about 50:50 (MFLM), predominantly MOM (>70%, PLM) and predominantly formula (>70% PFL). They showed a sort of dose response, this is a box and whisker plot of the number of OTU’s.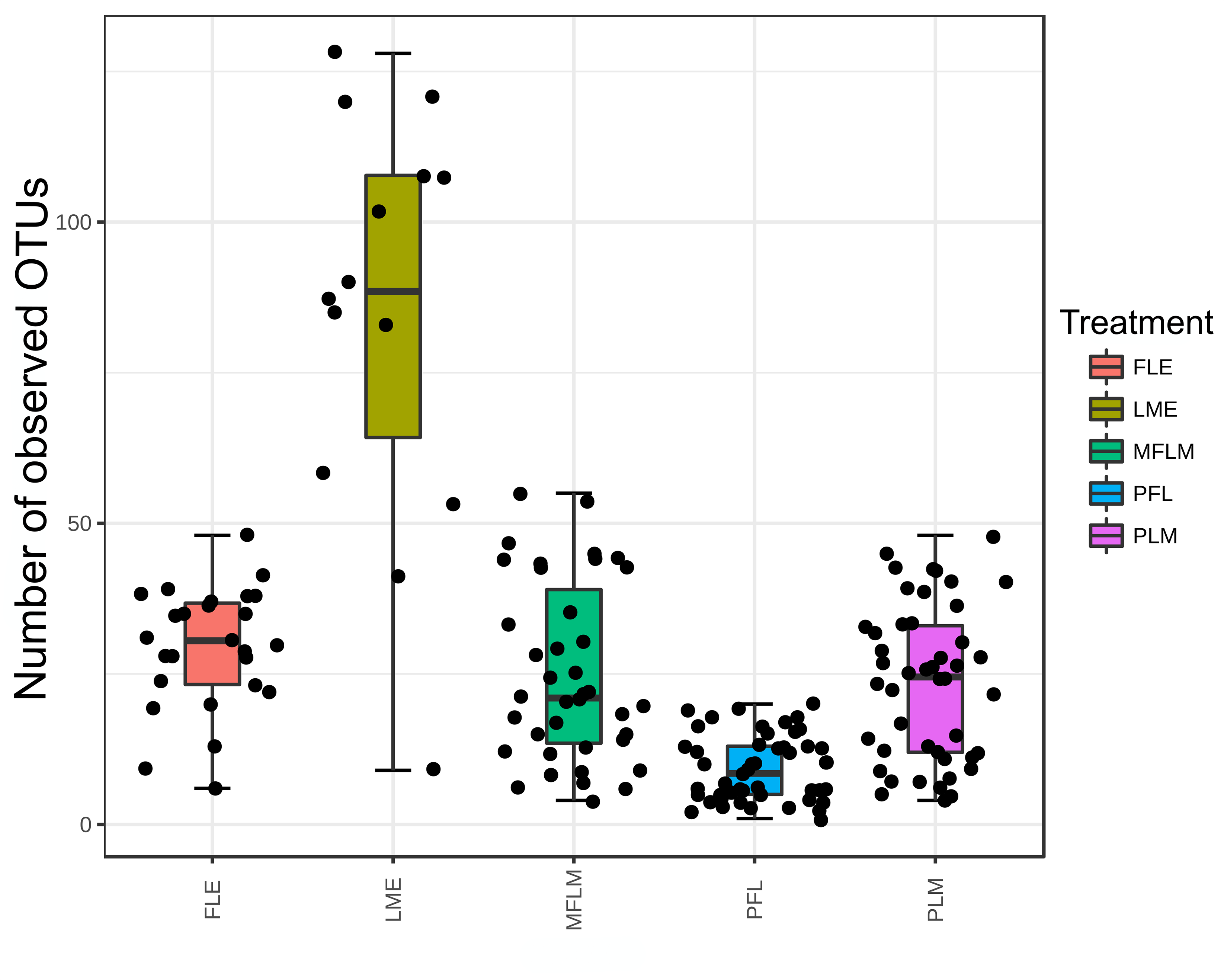
Figure 2: Number of Operational Taxonomic Units measured in fecal samples from preterm babies fed with different diets during 28 days.
Operational Taxonomic Units is a jargon used to avoid speaking about species, as the definition of a species among bacteria is not a settled issue, microbiomologists define an OTU according to the percentage of the bacterial DNA in the 16s RNA gene which is similar to others. In this study a similarity of 97% was required to define the OTU. So there are clearly many more OTUs, and more bacterial types, with exclusive MOM compared to other types of milk feeds.
This is their graph 1, showing the beta-diversity results.
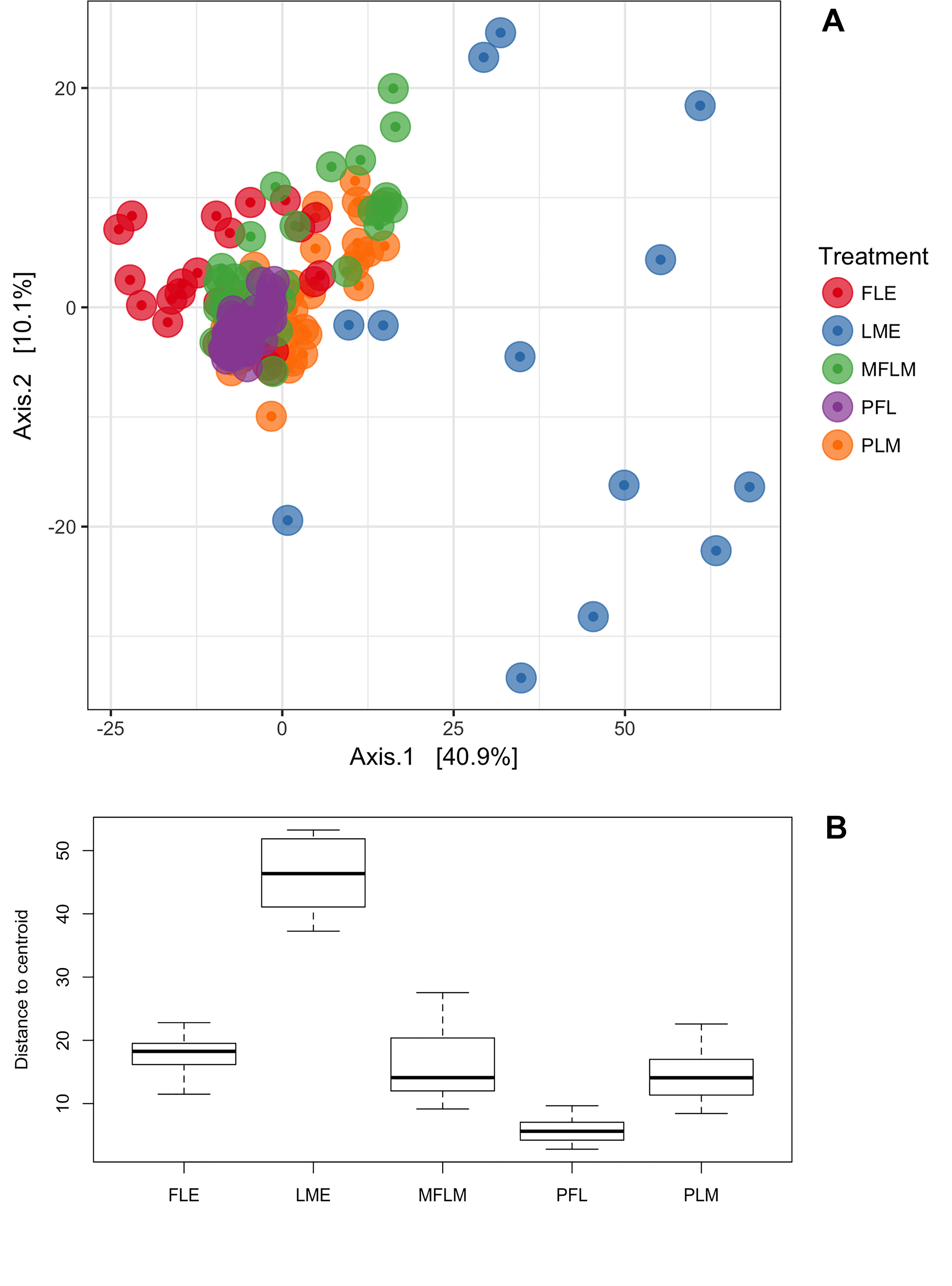
Graph A represents clusters of microbial communities. Each point represents an individual sample, with colors indicating feeding treatments. Graph B represents measurement of multivariate dispersion for each treatment.
You can see that the different feeding types tend to cluster differently, with the Exclusive MOM group (LME) the most different to the others. Interestingly, in this study the human milk was fortified with a powdered fortifier FM85 (personal communication Renato Procianoy) when the infants were at 80% of their full feeds, so the addition of the bovine protein-based fortifier does not seem to affect the microbiome diversity sustained by MOM.
Other studies looking at donor milk also show differences, with higher diversity when receiving MOM than when receiving PDHM. This might in part be because MOM usually contains bacteria classed as probiotics (particularly bifidobacteria), which are eliminated by pasteurization.
What does all this mean?
MOM is best, as usual.
Although we don’t know exactly why, MOM, which is not pasteurized or otherwise manipulated, supports a microbial intestinal community which is more diverse, and contains more bifidobacteria and lactobacillae than other milk sources. PDHM seems to have intermediate effects on NEC and on the microbiome, while formula feeding leads to major impacts on the microbiome and on the incidence of NEC.
Why does this matter?
If the adverse impacts of formula feeding are not because of the source of the protein, but due to other impacts of the processing of the milk on protein structure, milk composition, and the intestinal microbiome, then it is possible that we could produce an MOM replacement, and/or a fortification method which was able to support optimal growth without an increase in NEC. We should investigate ways of processing donor human milk which lead to less impact on intestinal function, so that when we don’t have enough MOM we can find a replacement that is just as protective.
Much more robust data on the safety of bovine fortifiers, comparison of liquid and powdered fortifiers, and proof of whether or not human milk based fortifiers are preferable, would help to maintain optimal nutrition while assuring the best outcomes for our babies.






