
After several years of preliminary investigations, a huge RCT has been published from India (Panigrahi P, et al. A randomized synbiotic trial to prevent sepsis among infants in rural India. Nature. 2017;548:407.) which enrolled babies over 2 kg birth weight between 24 and 96 hours of age to receive a synbiotic mixture, Lactobacillus plantarum with a fructo-oligosaccharide, which they received for 7 days. This followed studies showing that this mixture led to stool colonization for several weeks of life. All the babies were breast-fed, although a few received additional liquids by mouth, including water and honey.
The babies were then followed for up to 60 days to see if they needed evaluation for sepsis, which was diagnosed by WHO criteria. The primary outcome of the trial was the combined outcome of death or sepsis.
They planned to enrol over 8,000 babies, but stopped early after “only” 4,556 babies for efficacy.
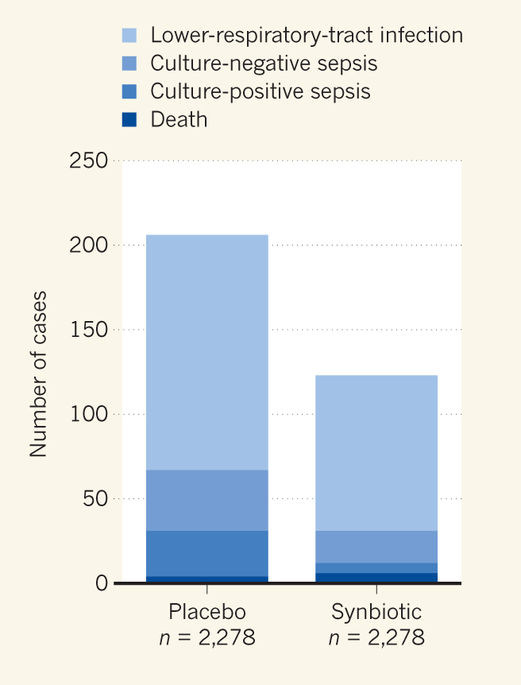
The combined outcome of death or sepsis was reduced from 9% in the controls to 5.4% in the synbiotic group. The entire difference being in sepsis, as mortality was low (<0.3%), there was a reduction in gram-negative sepsis, gram-positive sepsis and lower respiratory tract infections, as well as in culture-negative sepsis.
The study was a remarkable achievement, an individually randomized, placebo controlled trial in over 150 villages in India. The study excluded smaller babies, and those thought to be under 35 weeks, as well as 254 suspected to be septic at the time of screening for study entry, and those whose mothers appeared to have perinatal infections. The total number of exclusions came to 2,506. The synbiotics were supplied in capsules with “mixing containers and syringes with needles” initially kept at -20 degrees Celsius then distributed with cold packs. I am not sure exactly how the synbiotics were administered, which I think is an important detail for future wide implementation. I presume the syringe and needle were used to inject a solvent (?sterile water) into the capsules and then aspirate it prior to administering the liquid into the mouth of the baby.
The technical difficulties in distributing and administering this synbiotic preparation as a routine will need to be addressed, but this is an intervention with little or no risk that could improve outcomes for millions of babies around the world.






