
Many of our patients need invasive ventilatory support, for which endotracheal intubation is required, but we intubate many fewer babies than in the past. We also very rarely intubate babies for endotracheal suction to remove meconium any longer. Which means that there are vastly fewer opportunities for trainees to learn intubation. I never kept a log while I was training but I am pretty sure that I intubated more babies in my first 2 weeks on a neonatal service than residents now do in their entire training. In addition to the above factors, extended role respiratory therapists and nurse practitioners also need training and experience.
Training juniors and other practitioners to intubate is something I have done many times, usually by showing them the appearances during a laryngoscopy, and talking through the procedure as I performed it, followed by close supervision for a few intubations. It is difficult however, sometimes, to see what they are doing wrong (except when they pick up the laryngoscope with the wrong hand, for example).
There are now 2 RCTs of the use of a video-laryngoscope during the training of intubators in the NICU (one of which was done in my institution, the PI being my colleague Ahmed Moussa), and 2 recent crossover trials of using the video-laryngoscope during training in the simulation lab with mannequins (one of which was by the same Dr Moussa Assaad MA, et al. Learning Neonatal Intubation Using the Videolaryngoscope: A Randomized Trial on Mannequins. Simul Healthc. 2016;11(3):190-3) this is the other one Parmekar S, et al. Mind the gap: can videolaryngoscopy bridge the competency gap in neonatal endotracheal intubation among pediatric trainees? a randomized controlled study. J Perinatol. 2017.
The results are very consistent, trainees intubate with much more success during initial intubation attempt when using the video-scope, but they take a little longer per attempt; when they then attempt intubation with a conventional laryngoscope they maintain the skills that they learnt.
The two clinical trials also showed similar results, success on initial attempt was much higher with the video, this was despite difference in study design, in the study mentioned already the residents were randomized to using either the video-laryngoscope or a conventional scope, in the other trial they all used the video-scope but were randomized to having the screen covered or not the trainees did not look at the screen in this second study, the supervisor looked at the screen to give them guidance about their technique. The duration of intubation was a little longer with the video compared to the conventional, (Moussa et al) but identical between the video with screen visible and with screen hidden groups; O’Shea et al.
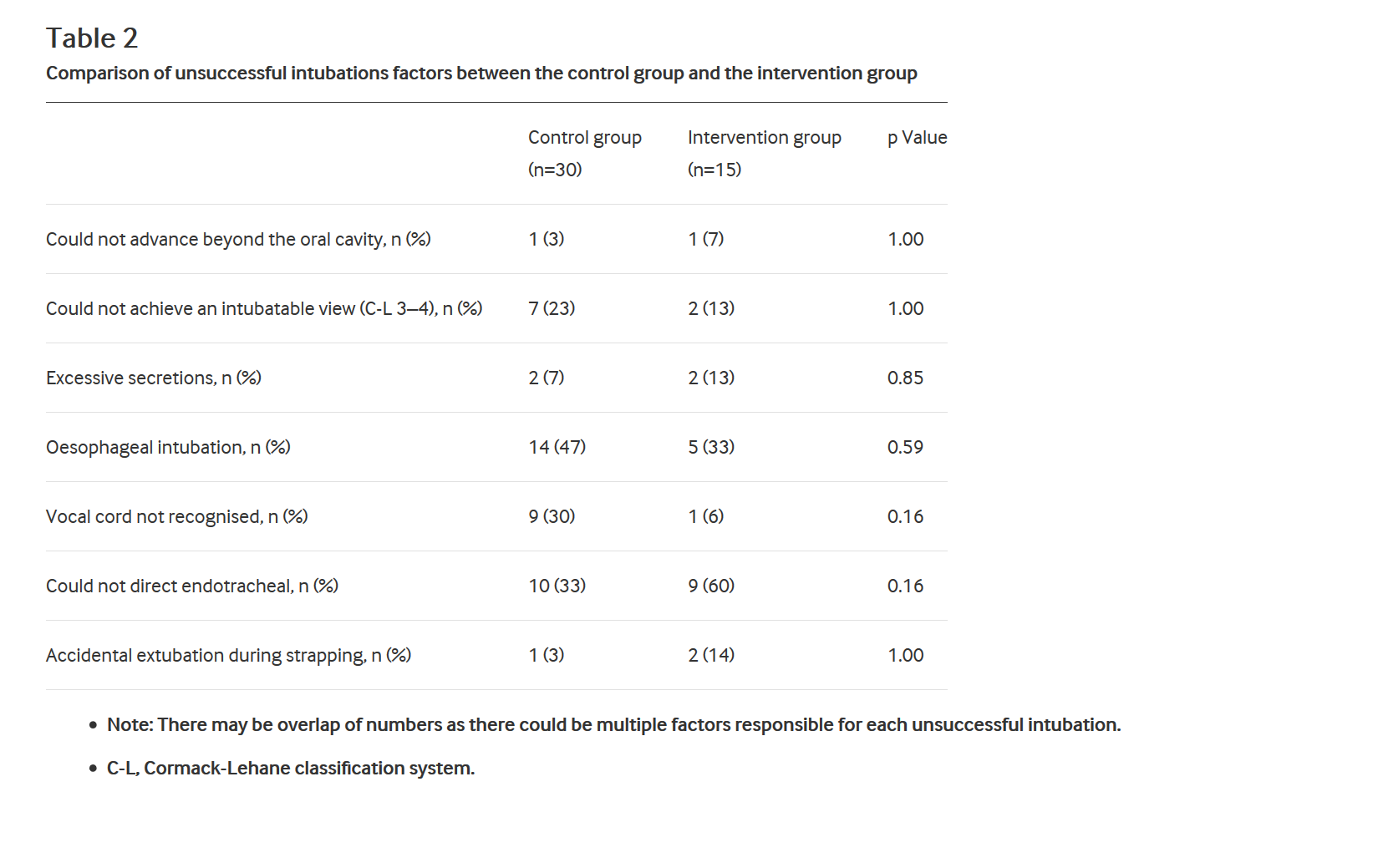
Why do trainees fail to intubate? I think we know the reasons why trainees fail to intubate, but the relative frequency of those causes, and how we can use video-laryngoscopes to reduce and correct them was, I think, unstudied. Until the remarkable Peter Davis (who seems to publish more clinically useful research than anyone else in neonatology, it is hard enough to keep up with the neonatal literature, Peter single-handedly makes it much harder!) and his group reported these data : O’Shea JE, et al. Analysis of unsuccessful intubations in neonates using videolaryngoscopy recordings. Archives of disease in childhood Fetal and neonatal edition. 2017. This is an analysis of video-recordings which were made of both groups in the above mentioned study, even the babies in the screen hidden groups had the videos recorded.
You can see here the categories of failure reasons in the 2 groups, which are similar apart from failure to recognize the vocal cords, presumably a supervisor watching the screen could say “look, there are the cords!” (to which the residents does not respond verbally, while thinking “oh, so that’s what they look like, why aren’t they yellow like in the text-book?”)
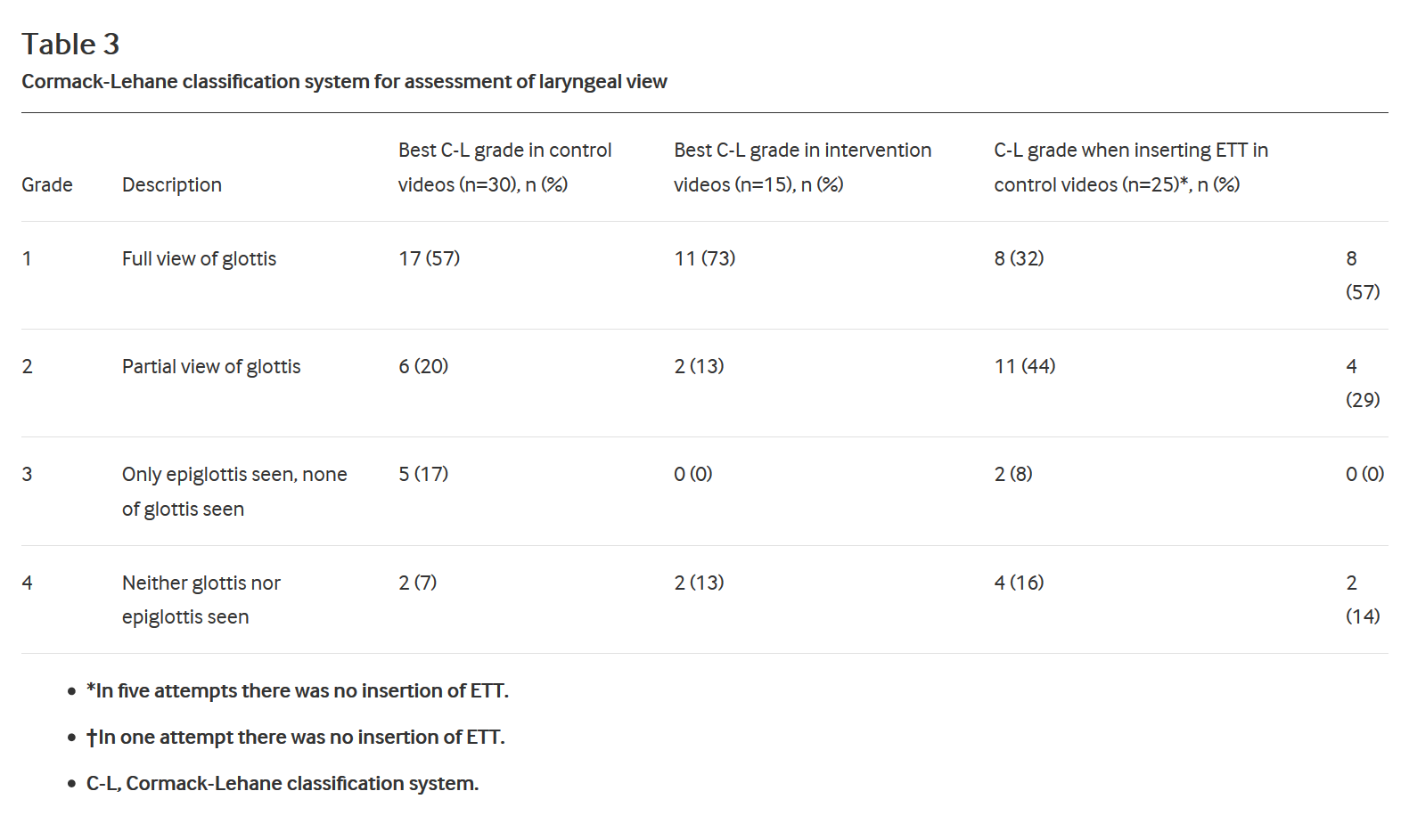
The degree of visualization of the glottis was analyzed, and the video-visible group (the intervention group) achieved better visualization, presumably because of the coaching. (of note there is a header missing over the last column of this table in the published version of the article, I presume the header says ‘C-L grade when inserting ETT in intervention videos (n=14), n%):
I think the video-laryngoscope is clearly an essential tool for teaching neonatal endotracheal intubation, you have to be aware that there are differences between the available devices, the 2 clinical trials highlighted here used different scopes, we use the Storz device, which does not have a 00 blade, and has a somewhat bulkier blade design than a standard Miller blade. Because of this I don’t use it for intubation below about 750 grams. As we don’t teach intubations on babies under 29 weeks that doesn’t cause a huge problem, but I would like to be able to demonstrate the anatomy on smaller babies, and I think even for more senior trainees with experience in intubating bigger babies, the capacity to use the video-scope for coaching in the littlest ones would be invaluable. The Melbourne group used a “Lary-flex” from Acutronic, with a blade which looks more like a traditional Miller blade, and has a 00 available.
As they note in their article, blade design, even among blades which are all named “Miller” differs between manufacturers, a fact of which I have had personal experience, when a hospital changed suppliers, as the alternative was cheaper and had the same appellation, but the blades were quite different and much more of a problem for intubating tiny babies.
Should all intubations be performed with a video-laryngoscope? In the NICU there is little good evidence about use of the video other than for training. A brand new systematic review of intubation complications and how to reduce them (Cabrini L, et al. Tracheal intubation in critically ill patients: a comprehensive systematic review of randomized trials. Critical Care. 2018;22(1):6) showed no clear benefit of video-laryngoscopy for routine intubation, or high risk intubations, and even a higher risk of complications compared to standard laryngoscopy. That is based on post hoc analysis of data from the 2 largest trials (out of the 9 total trials that they found, all in adults).
A review in pediatric patients from a few days ago (Xue F-S, et al. Paediatric video laryngoscopy and airway management: What’s the clinical evidence? Anaesthesia Critical Care & Pain Medicine. 2018) found a large number of articles in children, most of which either excluded newborns, or included very few of them. They were unable to find convincing evidence of the benefit of the video-laryngoscope in clinical practice, and noted the great variations between the 5 models they reviewed (which did not include the Lary-flex).
I think trainees should be taught to intubate using the video-laryngoscope, and, until they are clearly highly competent, all their intubations in the NICU, and perhaps in the delivery room, should be supervised by someone who is highly competent and experienced, and is reviewing the screen showing a video of the process.
Introducing the video for routine intubation of the newborn by individuals who are already experienced and highly competent is not currently supported by any good evidence, although my feeling is that with optimised equipment it may one day become standard of care. This may need further refinement of the equipment, and improvement in blade design, including availability of 00 blades for the tiniest babies.
Endotracheal intubation is associated with frequent adverse events, some serious. Improving the safety of our patients, while ensuring the competence of our trainees as they prepare for independent practice is essential.







This is an interesting topic and I agree with most of your comments.
We have purchased the Storz video-laryngoscope and used it over the last 6-7 months in our unit, even in 500 g babies using the 0 blade. We do not have frequent intubations with only 10-15 ELBW infants admittted annually. Thus, opportunities for training/teaching are limited.
The perception (no statistics!) among all neonatologists is that the view with the video-laryngoscope is much better (and obviously larger) than with a regular laryngoscope, and that intubations therefore become easier. Despite beeing comfortable with the regular laryngoscope we all feel that intubations with the video-laryngoscope is less “traumatic” and reduces the risk for repeated attempts. And you can very well see that the tube goes in between the vocal cords.
For me it seems fair towards the patients to use the best equipment available, also for more experienced doctors. Is it ethically sound to continue using “old” equipment when new and better equipment is available? Would surgeons do that?
Claus Klingenberg
Tromsø, Norway