
The benefits of human, especially mother’s own, breast milk are unambiguous, but is expressed breast milk as good as direct breast-feeding?
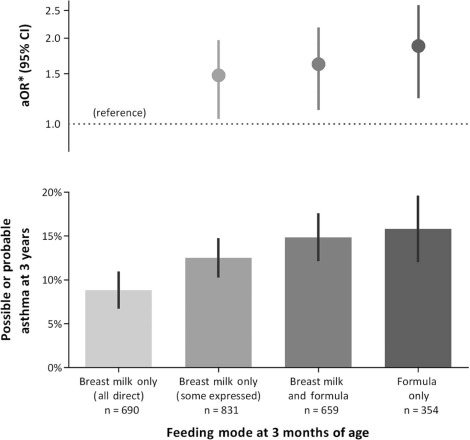
A new cohort study from Canada (Klopp A, et al. Modes of Infant Feeding and the Risk of Childhood Asthma: A Prospective Birth Cohort Study. The Journal of pediatrics. 2017;190:192-9 e2) suggests that, in terms of prevention of asthma among term babies, breastmilk is superior to formula, but direct breast-feeding may be superior to giving some expressed breast milk in a bottle. In this prospective study, mothers were questioned about feeding at 3 months of age, and infants were evaluated for definite or probable asthma at 3 years of age. Infants were divided into 4 groups, breast-feeding only, breast-feeding with some breast milk expressed and given via bottle, breast-feeding with some formula supplement, and formula feeding.
Obviously the mothers in the different groups were different, so an attempt was done to correct for the differences in socio-economic status, education, day care attendance of the baby and so on.
They showed a progressively increased prevalence of asthma across the 4 groups :
Is this likely to be true? These questions can always be asked about observational studies, what are the likely confounders, did the authors adequately correct for them and consider others, and is there a plausible explanation for the findings?
The division into breast milk direct only and “some expressed” seems to have been dichotomous, so a mother who expressed nearly all her breast milk, and another who did this once a day or once a week were all in the same group. As far as I can see, even one feed of expressed milk would qualify the baby to be in the second group. There are likely to be other undetected differences between mothers, and perhaps between babies, I can’t see any calculation of when mothers returned to work and why, how much the smoking-mothers smoked (there was a difference in smoking prevalence between groups, but no association with an asthma diagnosis, which seems a little surprising). There are probably other unknown factors also, which is always the case in observational studies.
Is it plausible? There are differences between freshly expressed breast milk and frozen thawed breast milk, for example, after 3 months of freezing lactoferrin has dropped by about 50%, freezing also kills living cells, including immune-modulating cells in breast milk, pretty quickly. (In contrast, freshly expressed breast milk in glass containers maintained in a domestic refrigerator seems to have little detectable difference to fresh milk). If these are really the potential mechanisms of this possible effect, then the more expressed milk is consumed, and the longer it is frozen should be relevant, the proportion of expressed compared to direct breast milk should be relatively easy to determine, although they may not have noted that in their original data sheets.
It seems inherently unlikely that an occasional feed (perhaps up to once a day) of expressed breast milk in a breastfed baby should have substantial impacts on the health of that baby. Perhaps majority expressed milk or exclusive expressed milk might have an effect which is different to occasional or minority expressed milk.
I think based on this we can say 2 things, encouraging breast-feeding, and making it feasible for new mothers to have several months of leave to breast feed their babies is important (USA, I am talking to you!) There may be an increase in asthma prevalence with mixed breast-feeding and expressed breast milk feeding, this may be due to unknown confounders, but, if causative, it is likely to affect those with the largest proportion of their feeds as expressed milk, however feeding some expressed breast milk which is still preferable to formula feeding.
What about the preterm baby? If a baby is too immature to go directly to the breast, it is clear that the best feeding is mother’s own milk, expressed, and handled appropriately. When possible, and if possible, direct breast-feeding helps, in general, to maintain good milk supply, other potential benefits compared to expressed, stored, breast milk are uncertain. A recent review of the data regarding breast milk expression and preparation has just been published (Picaud JC, et al. Review concludes that specific recommendations and stringent conditions are needed to harmonise the provision of fresh mother’s milk to their preterm infants. Acta Paediatr. 2018) The review seems quite extensive, and much of the interpretation is appropriate, but I must say I don’t agree with some of the conclusions as shown by the 2 algorithms at the end of the article. They state that any milk expressed at home and given to ELBW or extremely preterm infants (<1000g or <28 weeks) should be cultured and then pasteurized if there are pathogenic bacteria, in which they include staph aureus, which one study showed was found in almost 100% of expressed breast milk. In addition for the same babies, if the mother is IgG anti-CMV positive, or the status is unknown, then the milk should be pasteurized until the baby reaches 32 weeks.
I am not aware of any evidence of the efficacy of culturing breast milk, and then pasteurizing those with positive cultures, but pasteurizing breast milk has major impacts on its constituents, especially traditional Holder pasteurization. One randomized trial showed a trend toward increased sepsis among preterm babies who received routinely pasteurized compared to raw breast milk. If you use culture independent techniques, about 100% of breast milk is non-sterile (Jost T, et al. Assessment of bacterial diversity in breast milk using culture-dependent and culture-independent approaches. The British journal of nutrition. 2013;110(7):1253-62) and usually contains lactobacilli and bifidobacteria among other things, which will be destroyed by pasteurization. I think if selective culture and pasteurization and going to be used for expressed breast milk in high risk babies, there should be some scientific evidence that this is beneficial, which I cannot find, and the review by Picard does not reference. In fact the only evidence that they refer to that bacterial contamination of expressed milk is a significant hazard are from a publication about contamination of a pasteurizer with Pseudomonas (which is ironic) and a case report of triplets who became colonized with MRSA from mother’s milk. Other data show that milk cultures are not routinely helpful. There are occasional reports of babies becoming septicemic with organisms that can be found in expressed breast milk, but the disadvantages of pasteurization might well outweigh any potential advantage of eliminating pathogens.






