
We have also updated the Cochrane review of inhaled NO in the term infant. (Barrington KJ, Finer N, Pennaforte T, Altit G. Nitric oxide for respiratory failure in infants born at or near term. Cochrane database of systematic reviews (Online). 2017;1:CD000399). This was also a major update, with the addition of 3 trials, but also a restructuring of the review. On adding the trial from Gonzalez, which was a trial of early compared to late NO in 2 hospitals in Chile without access to ECMO, we re-thought several of the other trials that we had previously analyzed as being trials of NO which allowed backup treatment of the controls with NO. In fact there were 6 trials in total which had criteria for enrolment, and randomized babies to immediate inhaled NO, or to a control group who would receive inhaled NO if their oxygenation worsened to more severe criteria.
We have now analyzed those 6 trials (Barefield 1996; Day 1996; Sadiq 1998; Cornfield 1999; Konduri 2004; Gonzalez 2010) as comparisons of early compared to late intervention with NO.
The risk of bias figure, including all the trials, is below:
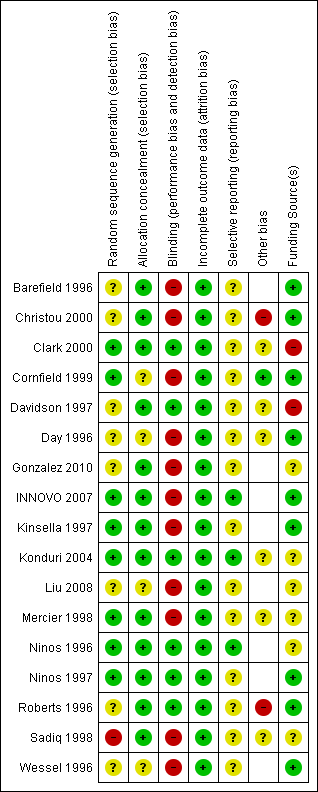
For several of the trials the funding source was not clear, hence the question mark, but for several which are marked by the question mark in yellow, including for example Konduri 2004, funding was primarily from a government granting agency, but there was also partial support from industry, with the manufacturer of inhaled NO providing the gas (and placebo) free of charge for the trial.
For the first comparison, inhaled NO versus control, studies which did not allow back-up treatment with NO in controls, the results of the analyses are unchanged. Inhaled NO is clearly beneficial in terms of reducing the need for ECMO, with an NNT of about 5.
We now present in the review a second comparison, inhaled NO at moderate compared to severe criteria for illness severity. The Summary of Findings table looks like this:

The actual criteria for illness severity were not consistent between trials, moderate severity was either based on Oxygenation Index (between 15 and 25, or 25 to 35 or 10 to 30) or on AaDO2 of 500 to 599. Whereas severe criteria were if they passed the upper limit of those ranges; so greater than 25 or 35 or 30 or an AaDO2 of 600 or more. I think there is enough overlap in the qualifying criteria that the studies satisfy Barrington’s rule, and that it is reasonable to meta-analyze them. But I realize that others may have a different response to that.
The overall message is that there is no proven advantage in clinical outcomes (death or needing ECMO) of starting NO earlier, compared to waiting for more severe criteria of illness severity. Fewer infants will progress to severe criteria if you start NO early, but if you wait until they become more hypoxic they will still respond.
There are, as always, some limitations to that statement, the confidence intervals are very wide, and include a possibility of a substantial relative reduction in mortality, (or a large increase). The absolute numbers dying, for example are 10% in the group who were treated at severe illness criteria, this might change to between 3.8% and 12.6% if the babies are treated earlier.
I don’t think based on these numbers that any promotion of the earlier use of inhaled NO can be justified. You will treat 100% of babies at moderate illness criteria, compared to treating about 60% of them if you wait for more severe criteria, which will have an impact on resource utilisation, but no evident impact on clinically important outcomes.






