
A new publication from a group of us in the CNN, suggests that the answer to that query is ‘not so fast’. Rabi Y, Lodha A, Soraisham A, Singhal N, Barrington K, Shah PS, et al. Outcomes of preterm infants following the introduction of room air resuscitation. Resuscitation. 2015.
Around 2006 most tertiary hospitals in Canada introduced room air resuscitation for babies at term. At about the same time many then changed their practice for preterm babies, either starting in 21% or at some intermediate concentration such as 40%. We used the CNN database for babies between 23 and 27 weeks gestation, to examine the likelihood of death or a severe brain injury (grade 3 or 4 IVH or PVL), during the 2 years up to their change in practice, which was not exactly the same in the different units. We then gave each centre a 1 year washout period, and looked at the same outcome over a later 2 year period with resuscitation initiated at lower O2 concentration.
We found that survival without brain injury was reduced after lowering the initial O2 concentrations, and that was true whether the practice was to start with 21% or with some other higher concentration. The adjusted OR was about 1.33, or a 1/3 increase in the Odds of the adverse outcome (that is after adjustment for all the relevant risk factors). There was about a 4% increase in the primary outcome variable, and about 3% increase in death and 3% increase in severe brain injury (of course, a baby could have both which is why 3 and 3 don’t add up to 4!)
Now of course, these are observational data, and observational data are always questionable, as a source of truth, or to direct changes in practice.
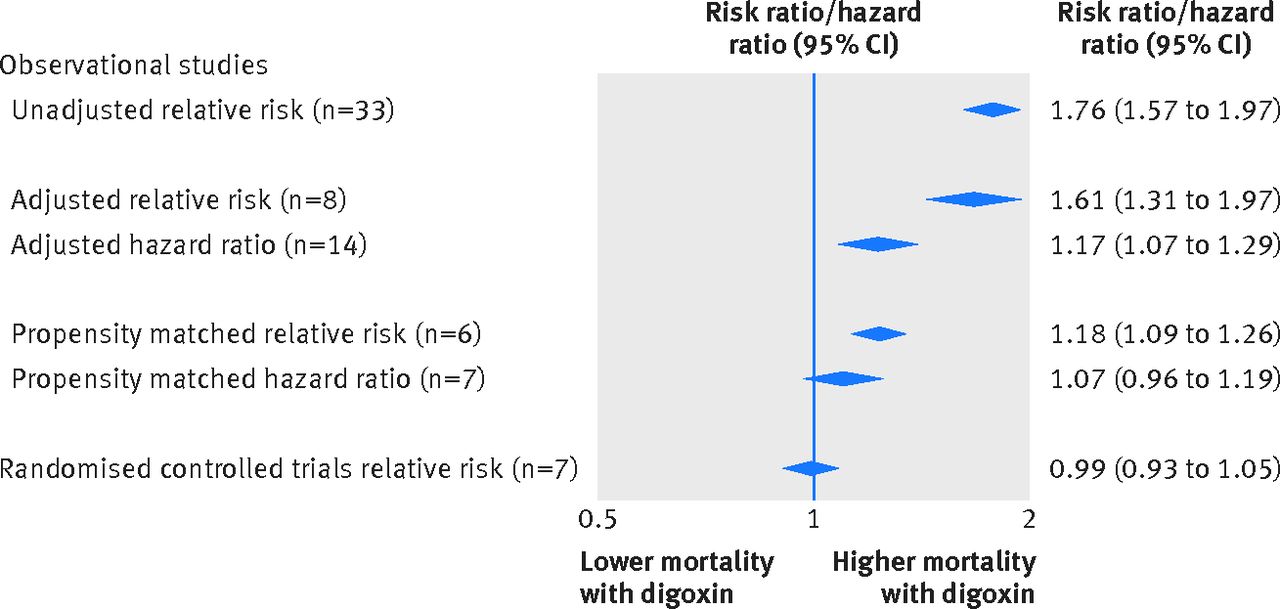
A new meta-analysis published in the BMJ is a great example of this, on a completely different topic. Ziff OJ, et al. Safety and efficacy of digoxin: systematic review and meta-analysis of observational and controlled trial data. BMJ. 2015;351:h4451. This was a review that compared the increase in mortality associated with treating congestive heart failure in adults with digoxin, between observational studies in 3 categories and the RCT data, the figure below shows a figure from their results.
As you can see observational studies show increased mortality with digoxin, in adjusted analyses there is less harm, in propensity matched analyses less harm again, and in RCTs no harm was shown.
A commentary accompanying the article has the great title, “trials are best, ignore the rest”
I guess, having just published the article with Jack Rabi, I should clarify what “ignore” means in that phrase. It doesn’t mean that the data we have just published are useless, it means that to make policy decisions, and to change medical practice you should ignore them. But for providing evidence that we should not make wholesale changes to practice based on the little data we currently have, and for providing support to do the trials that are sorely needed, I think they are worthwhile, indeed that is what we said at the end of that paper: “The contrast between the results of published systematic reviews and our observational data highlights the importance of performing adequately powered studies.”
The most important of the systematic reviews are those (here and here) which included only studies in preterm infants, they showed little detectable difference in outcomes between low oxygen and high oxygen groups, especially when studies without allocation concealment were eliminated.
On the other hand, studies like this one, Tataranno ML, et al. Resuscitating preterm infants with 100% oxygen is associated with higher oxidative stress than room air. Acta Paediatr. 2015;104(8):759-65 show much higher oxidative stress when babies were started in 100% oxygen and then titrated down, compared to being started in 21% oxygen then titrated up. This is data from a sub-study of the To2rpido study, of babies less than 32 weeks gestation, of whom about 120 had blood collection for oxidative stress analysis.
And, importantly the main To2rpido study was halted after the enrollment of nearly 300 babies because enrollment was very difficult and too slow. The interim results show a possible increase in mortality among the subgroup of babies less than 29 weeks gestation. Those interim results from an unplanned subgroup analysis (n=158), and our observational data, make a large prospective RCT an important priority.
It may be that the oxygen administration in those first few minutes after birth is very important for survival, and perhaps other outcomes of preterm babies. Even though oxidative stress is increased if you start with too much oxygen, adverse clinical outcomes might be worse with too low a starting oxygen. There really is only one way to find out.







Hi Keith – I suspect that what matters is not the FiO2 so much, but the PaO2 achieved. Resuscitation guidelines have recently changed such that relatively low saturations (and hence PaO2) are now accepted during the first 10 minutes. There is no evidence that such low PaO2 levels are safe in preterm infants. These low levels were extrapolated from the range of saturations observed in healthy term infants – a completely different population. It might be that a middle of the road starting FiO2 (eg 40%) allied with early application of sats probe and immediate targetting of sats 90-95% will avoid the twin perils of hypoxia and hyperoxia.
The posting raises the question of the relationship between prospective randomised trials, on the one hand, and other study designs on the other. It is not so clear cut. Sometimes, the observational studies all suggest the same thing. This was the case in the early days of ECMO, when observational studies helped refine the indications and led to widely held beliefs about the appropriate indications and contraindications for ECMO. A randomised trial than confirmed those results. (of course, one could ask whether one randomised trial is enough. After all, scientific theory would suggest that any positive trial needs to be confirmed to be valid. The real question is, when studies require the use of human subjects (especially non-consenting subjects), how much certainty or uncertainty is enough for us to say that it is either permissible or impermissible to randomise patients. What oxygen level would you choose for your preemies if he or she required resuscitation in the delivery room today? And would you be willing to randomised? From the evidence Keith presents, I think I would. But only because good non-randomised studies give conflicting results.
Hi Keith, thank you for going on with this blog
First, it is great to see this study published, we were waiting since its presentation at the 2012 PAS Meeting! And I totally agree with your comments on the interpretation of the evidence.
Second, in my opinion, while we still have uncertainties (we will always have some), I do believe it is difficult to justify a RCT comparing initial FiO2 of 0.21 vs 1.0 (I would avoid both as a starting point).
Third, I think there are problems both with high FiO2 AND high PaO2 (because of the pulmonary effects of hyperoxia)
Finally, it is not only FiO2 but also adequate FRC. Max Vento has shown that in (“healthy”) preemies receiving CPAP and RA in the DR, the SpO2 curve mimics the one on healthy term infants (Arch Dis Child Fetal Neonatal Ed. 2013; 98: F228-32)
I think a higher FiO2 could certainly cause oxidative injury in the lung, but to get more distal oxidative problems it would have to be followed by a high PaO2, which will of course occur, if you compare to the PaO2 of a room air resuscitation.
I guess one big question is what SpO2 curves we should be targeting? The best guess so far has been to follow the curves of preterm infants who adapt well, and who do well in the long term. But for fragile babies with immature lungs and circulation, is that the best answer? Maybe we should aim for something with a faster increase in the SpO2, such as Mike Hewson suggests,
That will be a tough one, and is really in addition to deciding whether we should start with lower or higher FiO2.
I agree with John that randomization is certainly a reasonable approach. I think that neither 21% nor 100% is likely to be the best answer, but the options in between are multitudinous. To2rpido has shown how difficult it might be to do such a study.