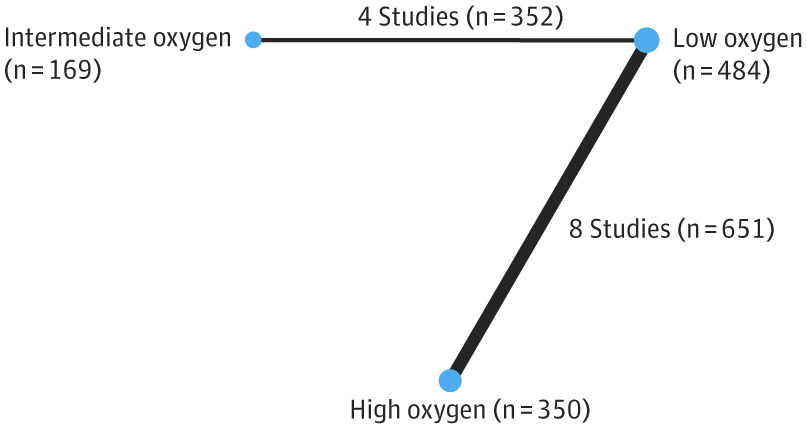
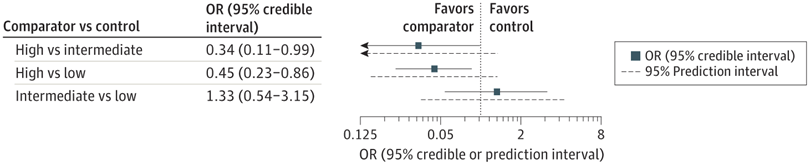
That NMA suggested that the higher starting oxygen groups (90% or higher), had a lower mortality than low starting concentration (30% or less), while intermediate, >30% to <90%, was similar to low starting concentration. Of note, the 1st TORPIDO study was the largest in that NMA.
Unfortunately, 10 of the 12 trials in that NMA were very small, 31 to 95 subjects, the 2 larger ones were modestly sized (287 and 193). For such an important outcome, and an easily applied, no-cost intervention, better, larger trials were needed.
The new TORPIDO 30/60 trial started in 2018, well before NETMOTION was performed. According to the choices made by the authors of NETMOTION, it would have been considered a comparison of intermediate (60%) to low (30%) oxygen. At the time of designing it, it was considered unlikely that very high starting oxygen concentrations would be a good idea, so the choice of a comparison between 30 and 60% was entirely reasonable.
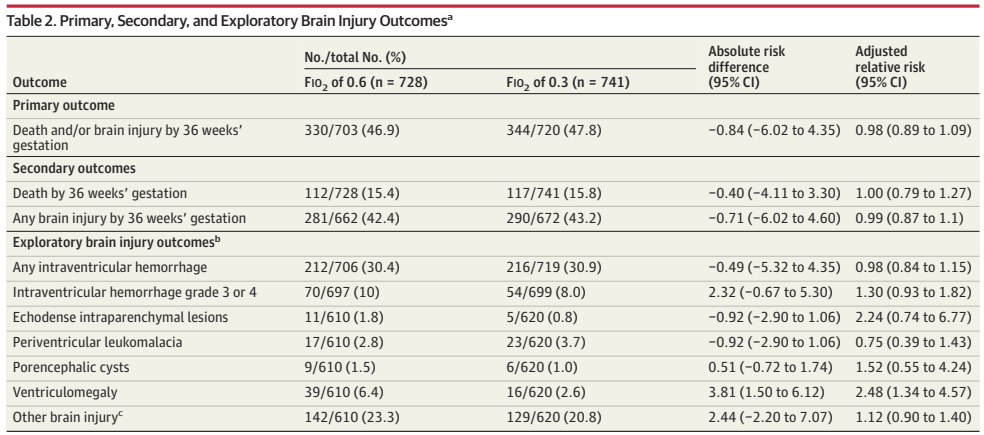
The new trial results show no difference in the primary outcome, or in any indices of brain injury on ultrasound.
There were some differences in immediate responses in the delivery room, “Newborns in the FIO2 of 0.6 group, compared with the FIO2 of 0.3 group, were less likely to receive chest compressions (2% vs 5%) or epinephrine (1% vs 2%) and more likely to reach SpO2 > 80% by 5 minutes (58% v 44%) (Table 3) and had higher initial SpO2.” Which are interesting differences, but did not translate to any measurable difference in clinical outcomes.
This suggests to me that we have to push this further, and compare a starting FiO2 of 60% (which seems no worse than anything lower, and might have some short term advantages) to a starting FiO2 of 90 or 100%. It seems weird, after all this time, to talk of going back to 100% oxygen for initiating resuscitation. It seems only a few years ago (but I guess it is more than 2 decades now) that I had to approach the hospital administration at my previous post to have pressurized room air and air/oxygen mixers installed in the delivery room, so that we could start resuscitation with 21%, and titrate if needed. The DR, in a relatively new building, had been built with just piped oxygen for neonatal resuscitation. The administrators of the Royal Victoria Hospital in Montreal were very responsive, and immediately approved the budget when I presented the evidence.
But if the data for preterm infants is taking us back to much higher oxygen concentrations, I guess we will have to decide whether 34 week infants should be treated like the 35 weekers, or like the more immature infants. Just like my comments about cooling, I think it is unlikely that the risks change dramatically at midnight between 34 weeks 6 days, and 35 weeks. We will need more granular information in order to make decisions for infants in the late preterm age ranges. Hopefully. those doing the trials will provide Individual Patient Data, that will allow analyses according to gestational age, and other risk factors.
It is over 2 years since I posted about this issue, in the meantime there have been a number of new initiatives, and several review articles and opinion pieces. Including a JAMA, “research of the year” article”.
I was triggered to return to this issue by a recent example of such an editorial which claimed that universal neonatal genome sequencing (UNGS) “pilot programmes like the Generation Study by Genomics England, which showed that whole-genome sequencing could identify rare, treatable conditions in about one in every 200 babies.” (Of note there is no author given for this editorial, perhaps it was generated by AI, interestingly a letter from a genomics researcher in the UK, in response to a letter to the editor, actually quotes this editorial as if it were reliable data from the project!)
This sounded to me to be a bit higher than previous estimates I have seen. Sometimes the supposed advantages of a Whole Genome Sequence have been dramatically overstated, for example, counting “referral to a pulmonologist” in the accumulated sum of benefits of screening. For large numbers of WGS performed in the NICU in sick infants, when there is actually a diagnostic result, the consequence has been redirection of care to comfort/palliative care, and sometimes the delay, waiting for the result, leads to a delay in redirection of care, when it could have been performed sooner without the WGS. For UNGS on the other hand, we really want to detect conditions in a pre-symptomatic phase which are amenable to intervention, and for which intervention improves outcomes, either survival, illness, or quality of life.
We also want to avoid false positives, that is detection of genetic variants that are abnormal, and associated with a disease, but do not cause the disease in that individual. The case of Krabbe’s disease, screened for in New York state, comes to mind. In nearly 2 million screens, positive results occurred in 620, of whom 346 had the genetic abnormality. Only 5 of them actually turned out to have infantile Krabbe’s disease, a PPV of only 1.4% for the disease among those who had the abnormal gene.
I decided to do my usual, and verify the source of the “treatable diagnosis in 1/200”, statement, and it seems that the authors (or the AI) have severely misinterpreted the results from Genomics England. That reference noted that, in the proposed 100,000 neonatal genomes they are accumulating, they are searching for a list of 200 different diagnoses, which they have selected as being candidates based on 4 principles. The principles are (a variation on the Wilson and Jungner criteria, which were modified to apply specifically to genetic screening): that a known gene is responsible for a disease; that the gene variant usually causes an important condition; that the condition is treatable when found on screening; and that all persons have access to treatment equitably. Which are principles that I think we can all agree with.
Other publications from Genomics England state that “fewer than 10% of rare genetic conditions have a treatment that is effective in improving patient outcomes”. (That isn’t referring to the conditions in their screening list, but in general). Of course, for several of the more common treatable conditions, universal neonatal screening is already in place (PKU, cystic fibrosis). What is the additional yield of treatable diagnoses, compared to standard screening? Surely that is the most important question, but I have had a lot of difficulty finding an answer. That is partly because standard screening is not standard around the world, but extremely variable, and the list of genetic conditions included as the targets in each program is extremely variable.
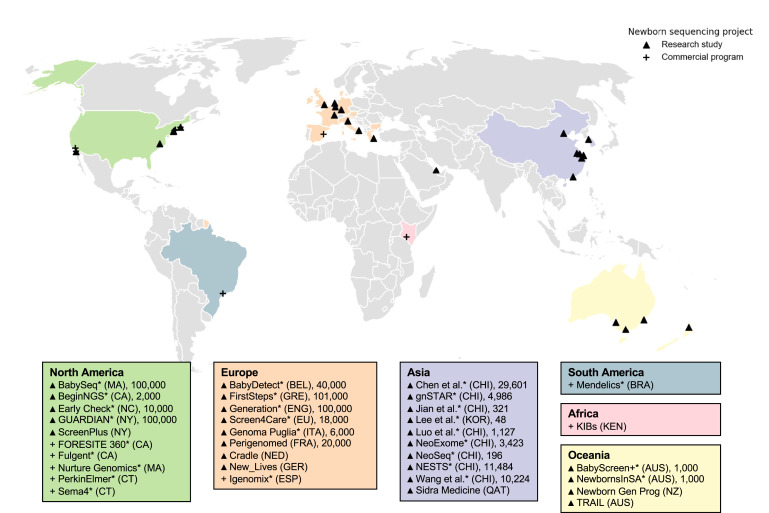
The various pilot studies, and there are now many, are also extremely variable, and have a diagnostic yield which is very variable, depending on which conditions are included, and usually do not state how many of them are actually treatable. Indeed there are over 30 current research programs into UNGS, as well 8 commercial bodies offering NGS if you pay for it (shown with the + symbol in the figure).
Of course, there may be benefits of a diagnosis, without an actual “treatment” as such. In one pilot, from Belgium, the largest diagnostic group, by far, was G6PD deficiency, which accounted for almost 50% of the positive UNGS results. That was a modestly sized study (about 3,900 babies included) with a diagnostic result in 71 cases, 44 of which were G6PD deficiency. The remainder were a variety of diagnoses with a variety of actions that were required. Four cases of CF, for example, 2 of biotinidase deficiency requiring biotin supplementation, and 2 of haemophilia with mild reductions in Factor VIII levels requiring intervention if they need surgery. There were several diagnoses that required enhanced specific surveillance in the future (cardiomyopathy variants for example).
The diagnosis of G6PD deficiency may indeed be a real benefit to the patient, who can avoid triggering factors for life, so I would count that as a potential benefit of UNGS; many screening programs, including in Quebec where I live, do not currently include G6PD. Indeed there are published standards which include the regulations in New York State where “public health law was amended to include quantitative diagnostic G6PD deficiency testing for infants with hemolytic anemia, hemolytic jaundice, early-onset increasing neonatal jaundice persisting beyond the first week of life (bilirubin >40th percentile for age in hours), admitted to hospital for jaundice following discharge, or familial or population risk for G6PD deficiency. G6PD testing is performed as a hospital diagnostic test, not by dried blood spot testing”. Does the detection of G6PD deficiency, by UNGS, confer an additional, measurable benefit to the infant, over such an aggressive case finding policy as that in New York?
One of the “publications of the year” in the JAMA group of journals, was the description of the GUARDIAN pilot of 4000 UNGS results. That study found 120 true positive results in the infants, of which 110 would not have been detected by traditional neonatal screening, 92 of those were G6PD deficiency. The remaining 18 infants include 1 with a fatty acid disorder (MCAD) 1 with achondroplasia (surely, a good physical exam would have picked this up) 1 with hypochondroplasia, 1 with Wilson’s disease, and 2 with prolonged QT. This study used a list of 156 “actionable conditions”, and there was a subgroup of infants whose parents consented to expanded testing including a further 99 conditions which were developmental disorders with an increased seizure risk. Among the infants who had that expanded testing they found a variety of disorders, total n=6, including, for example, 2 with different genes linked with Rett syndrome.
The large number of studies in progress is an indication of the uncertainty of the benefits. I also am very concerned about the potential for abuse in the future, with every infant’s genome sequenced in a database somewhere. My provincial government has just imposed a law which allows government officials access to everyone’s medical record. Ostensibly this is to improve co-ordination and access, but it is a serious intrusion into the confidentiality of medical records, and is being strongly contested by medical organisations here. Once everyone’s genome is recorded in a database, the potential for abuse is enormous.
The largest array of genes being screened for appears to be in BabySeq, with over 4000 genes in their list. Before instituting such a program as the universal norm, we have to be certain that the benefits, for the small number of infants who are detected by UNGS over and above the regular neonatal screening programs, outweigh the possible risks. A first step would be to determine whether detecting G6PD deficiency in asymptomatic infants actually improves their outcomes in some measurable way. The second step would be to analyse the outcomes of the 0.5% of babies who have another diagnosis, some of whom require follow-up, and some require a preventative intervention.
Most of the large programs around the world seem to be taking such a cautious approach. I am unsure if the commercial programs, whose primary motivation is profit, are quite as reasonable.
I have been continuing to think about this issue, so will subject you all to some of my thoughts. The large RCTs of medication for closure of the PDA show no benefit, and some evidence of harms, but we all know that the PDA usually closes shortly after birth in the term infant, and there is a statistical association between a persistently patent ductus in the very preterm infant and several neonatal complications.
So why don’t babies benefit from closure of the PDA?
I think there are 2 possibilities. One is that the medications are the problem. They are not very effective, and we expose the babies to reduced urine output, and other side effects, for unreliable constriction of the PDA, and a relatively small proportion of complete closure of the duct. Especially among the most immature babies, the drugs don’t work very well, and they have more secondary effects. Perhaps there are benefits to closing even modestly sized PDAs, but they are overwhelmed by the adverse effects of the medications we are using.
It is interesting that in the causes of mortality, as far as they can ever be definitively determined, there does not appear to be a difference in NEC, according to the meta-analysis that I referenced before, despite concerns of some that there may be an impact on GI perfusion of the meds. That SR/MA does, however, show an increase in severe IVH, PVL, and culture positive sepsis. None of which are individually statistically significant, but all of which suggest potential impacts that we often don’t consider. The decrease in urine output could also lead to an increase in lung water, ventilatory requirements and lung injury. So maybe the medications are the problem.
The other possibility is that the PDA is not etiologically linked to the associated complications, but is a bystander. I think for PDAs with a small shunt, this is probably the case. Centres with a very restricted approach to the PDA do not, generally, have worse outcomes overall. However, I think that is likely that there are babies who benefit from closure, including, perhaps, early closure.
Are there any babies, in controlled trials, who seem to benefit from PDA closure, in the current literature? Afif El-Khuffash and colleagues performed a secondary analysis of their trial which only included infants with a large shunt. The original trial publication (El-Khuffash A, et al. A Pilot Randomized Controlled Trial of Early Targeted Patent Ductus Arteriosus Treatment Using a Risk Based Severity Score (The PDA RCT). J Pediatr. 2021;229:127–33) showed a null result, but it was intended as a pilot trial, and was therefore under-powered for clinically important outcomes. The secondary analysis, was, therefore, even more underpowered, (Bussmann N, et al. Patent ductus arteriosus shunt elimination results in a reduction in adverse outcomes: a post hoc analysis of the PDA RCT cohort. J Perinatol. 2021;41(5):1134–41) there were only 17 infants who had successful closure of the PDA in the group with large PDA shunts who were randomized to treatment with ibuprofen. Among those who actually managed to close their PDA, they were better off than the placebo group infants in terms of “death or BPD”, 5/18, compared to 18/30 control group babies, which isn’t “statistically significant” by a simple chi-square. All secondary analyses are suspect, but, it does suggest that there may be a subgroup of babies who benefit from PDA closure. Interestingly, the active treatment group infants who did not close their PDA, were actually worse off (11/13 had “death or BPD), and possibly had more deaths.
One way of eliminating the adverse medication effects would be to close the PDA without medication. For those who are not aware, there is a trial in progress of ductal closure by catheter, the PIVOTAL trial, which randomizes infants of 7 to 32 days of age, <28 weeks GA, and over 700 g birth weight, who have a PDA score of 6 or more. The PDA score in use for this trial has been adjusted from that PDA RCT. I asked my good friend, the PI of the study, Carl Backes which score they were using and he very helpfully sent me this table, which I am sure he won’t mind me sharing.
PDA size indexed to weight= (minimum PDA diameter [mm]) / (weight [kg] at time of ECHO); IVRT=isovolumic relaxation time; PV=pulmonary vein; LA:Ao=left atrium to aortic ratio; LVO=left ventricular output; LV-VTI: LV output velocity time integral; RVO=right ventricular output; RV-VTI: RV output velocity time integral*obtain both LVO:RVO and LV-VTI: RV-VTI measurements; the highest score from either ECHO parameter is counted towards overall score*use the high suprasternal arch view to obtain the post-ductal diastolic flow measurement; reversal present from an abdominal view is acceptable, but the “absence of reversed flow” from an abdominal view may be a false negative, thus the need for the suprasternal view.
I hope that the PIVOTAL trial is planning a subgroup analysis by PDA shunt size or by gradations of the score, I think it is unlikely that a score of 6 or more was exactly the right choice, as the threshold for enrolment, but I could be proved wrong. The planned sample size was 240, and they are apparently about 75% complete. The trial will at least eliminate the problem of medication toxicity, but instead introduces the risks of catheterisation!
Catheter closure has rapidly been growing in the USA, the latest data I can find are from 2021, and they show things like the following, from the NICHD NRN
Indomethacin is disappearing, ibuprofen is relatively stable, acetaminophen has become the commonest intervention for the PDA, and the progressive disappearance of surgery is being replaced with the very rapid growth of catheter closure, being nearly 5% of babies born <29 weeks.
Given that there is an absolute lack of evidence that catheter closure of the PDA improves any clinical outcomes, it is very depressing to see that 1 in 20 extremely preterm infants in the NRN are being subjected to this procedure, almost all of them outside of any clinical trial.
Equally depressing the “Society for Cardiovascular Angiography & Interventions” (SCAI, a new one for me) have just published a position statement with a pre- and post- procedure checklist. Carl Backes, and his co-author wrote an accompanying editorial and they were much kinder about this position statement than I would have been. My response would have been : WTF? How can you write a position statement for a procedure completely lacking in supporting evidence that it is effective or safe, in terms of clinically important outcomes? Surely the position statement should have stated, that this procedure should not be performed outside of a prospective study.
Hopefully the PIVOTAL trial will prove to be pivotal, and will have a clear result, of benefit or no benefit. The primary outcome is ventilator free days, a reasonable way of analyzing the impacts on ventilator dependence or death (as deaths will be counted as 0 VFDs). Although I would have wanted other outcomes, in particular some evidence that effects on lung injury, using measures that are important to families, are improved, without an increase in mortality.
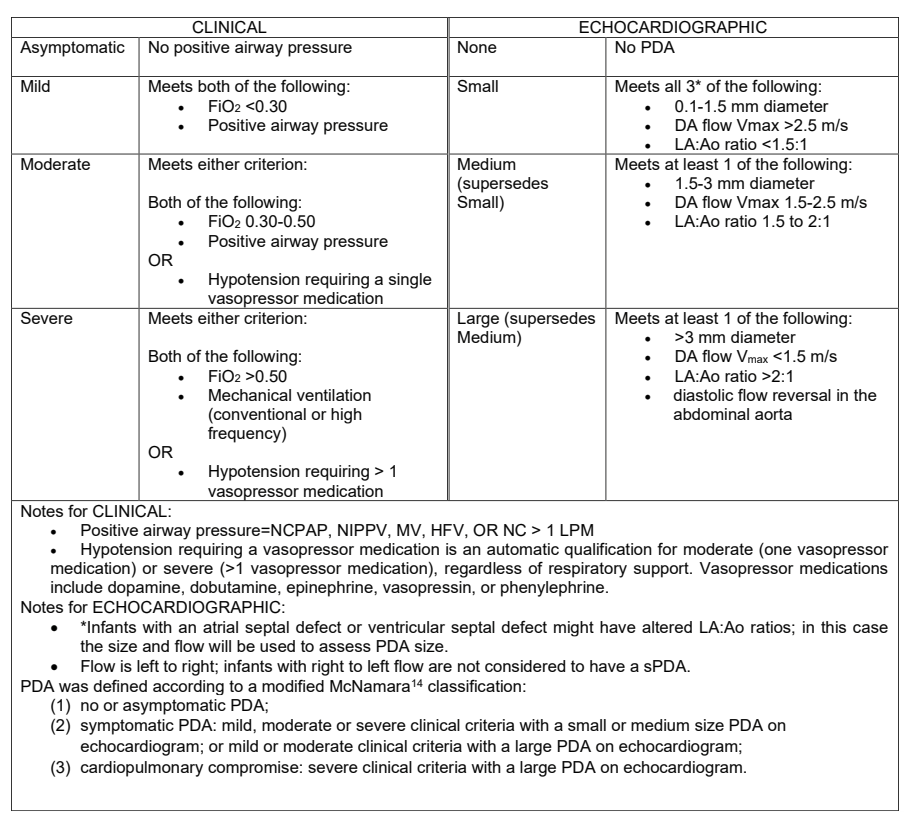
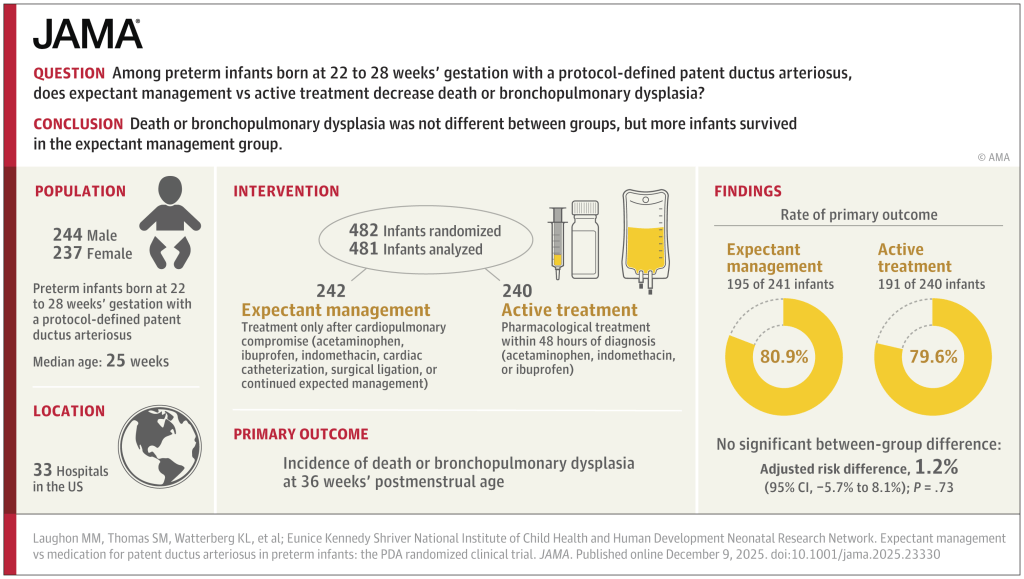
The latest large multicentre RCT has just been published. Laughon MM, et al. Expectant Management vs Medication for Patent Ductus Arteriosus in Preterm Infants. JAMA. 2025. In this trial, infants of 22 to 28 weeks GA were randomized at between 48 hours and 21 days of life after an echocardiogram. They were classified into: 1. no or asymptomatic PDA; 2.symptomatic PDA; or 3. cardiopulmonary compromise. Only group 2 were randomized. The definitions are shown below, including, at the bottom of the figure, the definition of group 2. Of note, infants receiving hydrocortisone were ineligible.
481 infants were randomized, within 48 hours of being eligible, and at a median of 10 days (IQR7-14) of age to either medical treatment, with ibuprofen, indomethacin or acetaminophen, or to control, expectant management. Controls were not supposed to receive any of those drugs unless they progressed to group 3 (cardiopulmonary compromise) or reached 36 weeks. There were unfortunately a large number of protocol violations, 60, or 25% of control, expectant management, infants received medical intervention (or surgical/catheter closure) for their PDA, of which 44 did not meet the agreed treatment criteria, and were therefore protocol violations.
I find this a little hard to understand, why get involved in the study if you are not prepared to abide by the protocol? Nearly 1 in 5 expectant group babies had PDA closure attempted even though they were not in the category of having severe clinical criteria with a large PDA, and therefore did not satisfy the protocol indications for treatment.
The primary outcome criterion was survival without BPD. I know, don’t get me started, designing a trial with a dichotomous outcome, that equates death with being in oxygen at 36 weeks, would be ridiculous in this day and age, in 2025, when so much better ways of designing trials with potentially conflicting outcomes, and analysing them in ways that take into account the relative importance of the outcomes, exist, and are now being used in other fields. It also leads to other rather, er, questionable decisions, such as defining death as death up to 36 weeks PMA. Really? Who cares about death up to 36 weeks, so an infant who dies at 37 weeks wasn’t counted in this trial?
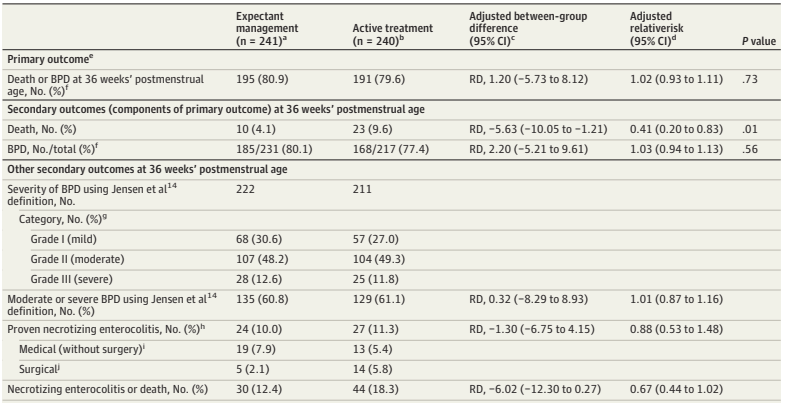
The trial was, strictly speaking, a null trial. The primary outcome was identical between groups.
The breakdown of the primary outcome shows a lower mortality with expectant management than with intervention. At least, that is, mortality up to 36 weeks.
Surely the most important single question about any trial in sick preterm infants is : “If the baby receives treatment for the PDA, compared to expectant management, are they more likely to go home alive, or not?”
It takes a search of the supplemental materials, supplemental document 3, eTable 9, to find a partial answer to that question. The answer is that, by discharge or transfer, or 120 days after randomization (there were 18 infants still in the NICU at 120 days, and the investigators terminated the data collection), there were 14 deaths of the 241 expectant treatment infants. In the active treatment group there were 26 deaths among the 235 who actually got active treatment, there were 5 babies in this group who were not treated within 48 hours, and we don’t know if they survived or not.
If I do an ad hoc ITT chi-square, removing the unreported infants who had data collection truncated at 120 days, (as we don’t know if they lived or died) then the mortality is 14/237 vs 26/234. Or 5.9% vs 11.1%, a risk difference of 5.2% (95% CI of -0.2% to 11%), in other words not “statistically significant”.
As regular readers will know, I don’t think the arbitrary cutoff of p<0.05 is a good way to define what is real or not, which is why I almost always put “statistically significant” in quotation marks. But still, surely it was important to know that there were 7 pre-discharge deaths, at least, of the 40 total deaths, that occurred after 36 weeks. And there may have been more deaths after 120 days.
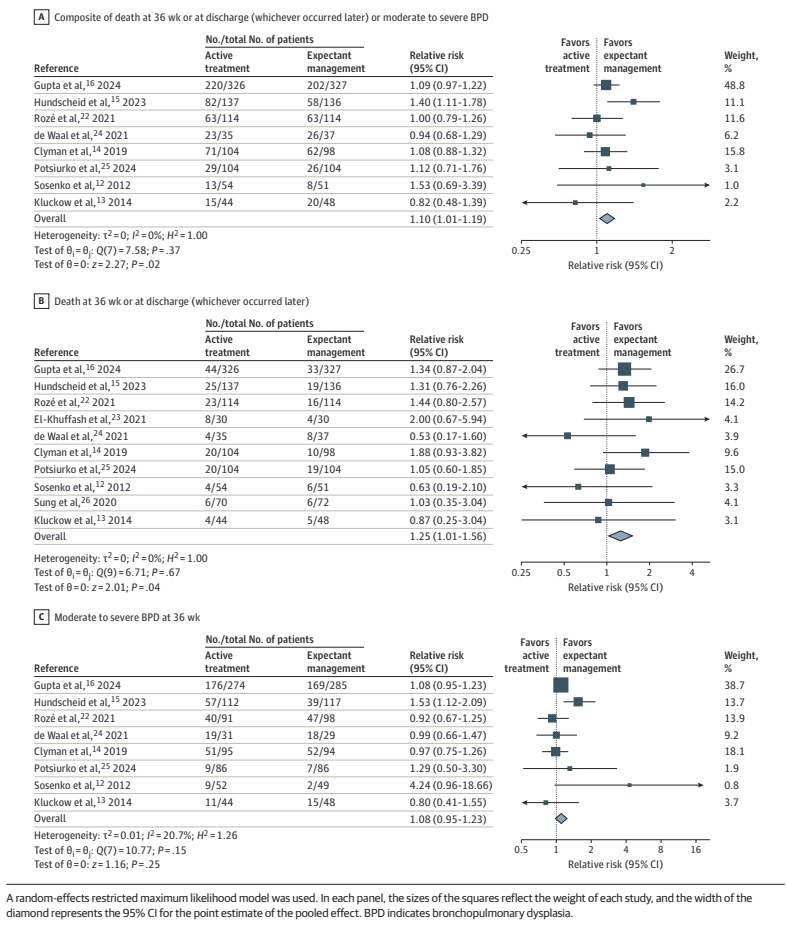
This has been a recurrent problem in similar studies, in BabyOscar for example, (Gupta et al 2024 in the figures below) mortality was reported at 36 weeks, and I can’t find any data anywhere about survival to discharge.
This is vitally important, the most recent meta-analyses show that medical treatment of the PDA increases BPD. Infants with severe BPD, still ventilated at 36 weeks have a measurable late mortality. Surely that is an outcome that we should know about?
As you can see, this analysis suggests that there may well be an increase in “death at 36 weeks or at discharge (whichever occurred later)”, by which they actually mean whichever were the latest reported mortality figures.
They also include in the secondary outcomes, mortality before discharge, reported for less than half of the babies included in the various studies, which also shows an increase, but less marked, and with 95% CI including no difference.
To return to the new trial publication. I should make it clear that the trial was started in 2018, therefore probably designed in 2016 or so, and the authors are the brilliant Matt Laughon and the NICHD NRN centre representatives. The outcomes that they chose back then were the typical outcomes of PDA trials. It is easy for me, tapping away for my blog, to criticize, in retrospect, decisions that were taken a decade ago…
Nevertheless this trial, if you add it to the meta-analysis above, would surely confirm that closing a “haemodynamically significant” PDA does not appear to have any measurable benefits, and may well increase both mortality and oxygen requirements at 36 weeks, with most of the increase appearing to be in milder BPD, but probably a small increase in more severe disease also.
I am struggling to think of an evidence-based indication to close the PDA in a preterm infant. The data are, unfortunately rather muddy, there have been many protocol violations in the majority of the large trials. The exception was Hundscheid et al in the figure above, the BeNeDuctus trial, which only had 1 protocol violation in the expectant group. In BabyOscar, in contrast, 30% of the placebo group received open label medical or surgical PDA closure, about 1/3 of whom did not satisfy the protocol defined criteria. In the Rozé trial, 62% of the placebo babies had open label treatment, it is not clear how many satisfied their criteria for open-label treatment.
Which brings me to the question in the title, “Is there any indication for PDA closure?” The evidence-based answer to that question is that there are no criteria for defining a clinically important PDA, for which medical or surgical intervention has shown a survival benefit, or a reduction in lung injury.
That recent opinion piece suggested that the criteria that should be used are those being tested in a pilot trial, the “Smart PDA” trial, which are not enormously different to the criteria used in the NICHD trial above. The authors of that piece remark that simply defining a significant PDA by diameter is insufficient; some PDAs with a large diameter have relatively modest impacts, and others of the same size may be associated with major shunts. The big difference between the Smart PDA trial, and the newly published NICHD RCT is that, in the newly published trial, being on CPAP, and having a PDA of over 1.5 mm would qualify for enrolment, without any other signs of a large shunt. In Smart PDA, you will also need at least one of the following signs of a L-R shunt
Left atrium: aortic root ratio 1.5–2.0
Transductal peak systolic velocity 1.5–2.0 m/s
Left ventricular output (ml/kg/min) 200–400
Diastolic flow pattern in the descending aorta: Absent/ retrograde
It seems to me that this has to be the next stage in the process, we should stop treating PDAs that do not have signs, such as those, of a substantial L-R shunt, doing so seems to have no benefit, and may well increase both oxygen requirements at 36 weeks, and perhaps even mortality. I think we have now reached the point where medical or surgical closure before 36 weeks PMA should only be attempted, in the context of an RCT, in infants with signs of a large shunt. There is currently no proven benefit to early PDA closure, and only harms.
In my recent practice I have seen some babies, usually “older” infants still ventilator dependent near term, with large shunts from a PDA, who have improved rapidly after ductal closure. In an NICU with 100 extremely preterm babies a year, there were maybe 3 or 4 in the last 4 years. It may be that those infants would have benefited from earlier closure, but in the absence of clearly defined criteria, which have been shown to predict benefit in preterm infants with a PDA, we frequently hesitate before performing a procedure with known risks. We have also had babies who have had little change in their clinical status after late PDA closure.
There do seem to be some babies who, anecdotally at least, seem to benefit from closure of the PDA. Our challenge as a community is to identify them, and hopefully to be able to identify them early enough that we can improve their outcomes.
There are many ways that an article in the medical literature may not be worthy of trust, and whose results may be unreliable. I remember one of my own trials, LACUNA, which was a pilot RCT of lactoferrin supplementation to prevent late-onset sepsis (LOS). As a pilot. the primary outcome was feasibility of a larger trial, but the clinical outcomes that I reported included the incidence of culture-positive sepsis. I calculated that as planned, as the proportion of babies who had at least one episode, out of the total number included in each group.
When I looked at the data, I realized that if I presented the results as infections per 100 patient days, there was actually a statistically significant difference between groups! I must admit to being tempted to report that outcome, as if it had been the primary outcome of my trial. I think the trial would have had a greater impact than it actually did, and could potentially have led to widespread adoption of lactoferrin as prophylaxis against late-onset neonatal sepsis. I could have been famous!
I am glad I resisted the temptation, because I know that it is vitally important to follow the trial design, outcomes, and statistical analysis that are planned prior to the trial. Any new analysis, or redefinition of outcomes, which is decided after examining the data, is inherently, extremely unreliable.
If I had reported that outcome, probably few people would have realized that I had changed the definition after performing the trial. The trial was pre-registered, but few people look at the registration documents, or compare the reported outcomes to those which were pre-planned. That includes peer reviewers, and meta-analysers.
It tuns out, of course, that the lactoferrin preparation that we used almost certainly has no real impact on LOS, and if I had reported the other outcome, it would eventually have been proven to be a red herring.
I was stimulated to think about this issue, which reminded me of the LACUNA outcomes, by a post from the Health Nerd https://gidmk.substack.com/p/the-terrifying-problem-of-fraud in women’s health. It is a really interesting blog, in general, and this post is indeed terrifying. He refers to several Cochrane reviews, including 2 that have major neonatal implications. He starts by discussing an influential Cochrane review of vitamin D supplements in pregnancy, that, in previous versions, was very positive, and led to recommendations from various health groups to give such supplements. He notes that the new version of the review has removed 21 articles because of trustworthiness issues. Twenty-one! The review now shows no benefit, and, in fact, potential harms.
A review with major neonatal impacts is the Cochrane review of steroids prior to Caesarian Delivery at term. The previous version included 4 trials, with nearly 4000 babies, and showed some significant benefits. The new version has removed 3 of those trials, for being untrustworthy, and now only shows a possible reduction in NICU admission among the 900 babies included in the 1 remaining trial, but not in RDS, or respiratory support. That single included trial did not report hypoglycaemia, which other trials, in late preterm infants, have shown to be a major potential complication of steroids in that population. Based on this new Cochrane review, I think such use of steroids is highly questionable.
Another Cochrane review from the obstetric group with a neonatal impact is their review of sildenafil and other NO pathway medications for fetal growth restriction. The initial search identified 19 studies, but 11 had to be excluded because of trustworthiness issues. Even one of those included was not prospectively registered, so they performed a sensitivity analysis excluding those data. Only sildenafil had enough data to be informative, and the review shows no benefit.
It is now essential that systematic review authors evaluate the trustworthiness of the trials being included. Almost all journals state that they follow the ICJME guidelines, which preclude the publication of trials which are not pre-registered. On many occasions however, I have seen articles published that are reports of clinical trials, but do not mention registration, or were retrospectively registered. Systematic reviews often include data from those trials without commenting on the issue. There should always be a sensitivity analysis excluding unregistered or retrospectively registered trials in a SR. The SR of erythopoietin for prevention of NEC, that I discuss in the post linked below, went from showing a reduction in NEC with erythropoietin, to a null effect when the retrospectively registered trials were deleted.
Just like my example above, untrustworthy research is not necessarily fraudulent. It may be a minor twist to the definition of the outcome, or deciding post hoc, that a certain observation is an outlier, or changing the analysis from treating a value as a dichotomous to a continuous outcome. Sometimes, of course, there is overt fraud, with entirely imaginary numbers. The pressure on individuals in some countries to produce published research is so enormous, that there is no consideration of the downstream harms that can be caused by such fraudulent results. Or by results which are “tweaked” to show a benefit.
The problem of untrustworthy published research is not new, but I fear that it will continue to grow, with articles now being generated entirely by AI. The least we can do is to demand that all published RCTs are publicly registered, in a database including projected sample size, eligibility criteria, and primary outcomes.
Those of us performing systematic reviews must now perform trustworthiness assessments, using one of the published tools. It substantially increases the workload involved, but will also improve the reliability of the results.
“families affected by HIE remain sidelined in advocacy and institutional representation. We are routinely excluded in neonatology priority setting, where patient stakeholders may be represented, but HIE voices are not. The exclusion of HIE families leads to research agendas that don’t reflect our questions, timelines that don’t reflect our realities, and policies that fall short of what our children and families need.”
I think she has a point, many of our current parent partners are families of preterm infants, understandably, as they often spend weeks or months with us. HIE babies usually have shorter stays in the NICU, but the impacts on the families are just as great, and the long term impacts are sometimes greater. We should make extra efforts to ensure their voices are heard. She also points out some of the deficiencies of the longer term follow up of these children
“some families access follow-up to age two or three, very few have support as their children enter school, face academic challenges, or develop seizures, behavioral challenges, anxiety, or sensory processing issues. Research continues to overemphasize early developmental scores through assessments that are showing to not be predictive of neurocognitive development later in childhood when administered at age 2 or 3, and underemphasize the very issues that families identify as most critical in daily life”.
Any regular reader of this blog will know how much I agree with the limitations of early behavioural screening tests. Longer follow up of these infants is essential to both get a better picture of the impacts of HIE, but also to help the families to find the resources they need.
She ends with the following :
Max is now thirteen. He’s full of curiosity, humor, and resilience. He plays basketball, loves sushi, and is fiercely proud of how far he’s come. But he’s still living with the effects of HIE. We all are. Our journey didn’t end at discharge. It’s ongoing—and so is the work. Let’s keep going, together.
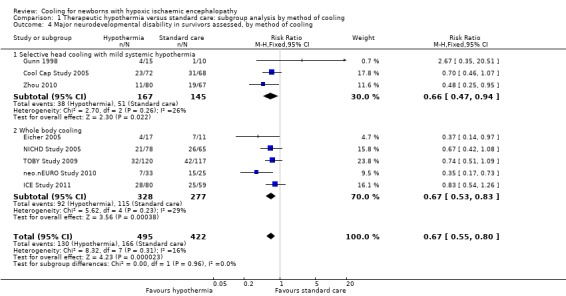
One of the numerous major advances in neonatology during my career has been the introduction of therapeutic hypothermia for infants with Hypoxic Ischemic Encephalopathy (HIE). Mortality is decreased, by about 25%, and long term morbidity among survivors is also decreased, by about 33%. Those estimates of effect size come from the Cochrane review, which provides the following Forest plot (I’m sorry about the quality of the image, the version in the pdf of the review is much clearer, but it extends over 2 pages, with a page break in the middle).
The Cochrane review also analyzed the impacts of cooling after dividing the infants according to severity of HIE, confirming that moderate and severe HIE both benefit. Unfortunately, the long term outcomes have been reported mostly up to 2 to 3 years. In the Cochrane review, 6 year outcomes are only available for the NICHD trial, which reviewed 120 survivors at 6 years, CP, IQ <70, executive function score <70, and moderate/severe disability were all lower in the hypothermia group than the controls, but the differences were small (and not “statistically significant”). The Cochrane review dates from 2013, and in 2014 the TOBY trial from the UK published follow up to 6-7 y of age, they showed more babies surviving without disability in the hypothermia group and “Among survivors, children in the hypothermia group, as compared with those in the control group, had significant reductions in the risk of cerebral palsy (21% vs. 36%, P=0.03) and the risk of moderate or severe disability (22% vs. 37%, P=0.03)”. Executive function scores were also higher in the cooled babies, and full scale IQ was 5 points higher (NS).
Scores on motor function scales were progressively worse as the children aged. Behavioural problems became more prevalent. Cognitive scores were overall fairly stable, but there was a progressive decrease in cognitive scores in the subgroup of infants who had damage to the mammillary bodies on MRI.
The changes were all due to deterioration in cognitive scores : “no further CP, epilepsy, or ASD diagnoses were made, cognitive performance declined in 11 children (28.0 %; p = 0.002; Wilcoxon test)”.
These studies point out the importance of much longer follow up of these children. They are an interesting contrast to preterm infants, who, overall, tend to have improved scores on standardized tests over time. The data on behavioural issues from the Dutch study, particularly increased internalizing behaviours, was interesting to me, as I was not really aware of this as a problem after HIE, also, behavioural problems are really important to families, and they may also be amenable to interventions to improve them.
These data make me wonder about the 2 issues of mild asphyxia, and the late preterm infant. If the prevalence of adverse outcomes changes so much over time, it may be that our decisions about which babies to cool are being influenced by somewhat unreliable data. There is very little longer term outcome data from the RCTs of cooling, to 5 to 6 years and beyond, that we might be missing a measurable benefit of cooling in such subgroups.
It is vital that trials of cooling for HIE, in groups for whom it is not yet proven to be beneficial, continue to follow the participants at least until early school age, and preferably towards adolescence. Only then will we be able to develop reliable data on the risks and benefits.
An excellent acronym for this trial. Hopefully it will lead to a trend in acronyms based on European culinary specialities. Very preterm infants, n=151, of 23 to 32 weeks GA were randomized to receive delivery room CPAP with a face mask, or with a nasal mask in a single centre study from Monash in Melbourne. Delayed clamping was attempted, without respiratory support, or immediate clamping if the baby needed intervention. If the baby needed positive pressure ventilation, that was delivered by face mask, the same in the two groups. When the babies could be placed on CPAP, they randomly had either a face mask placed, or a nasal mask.
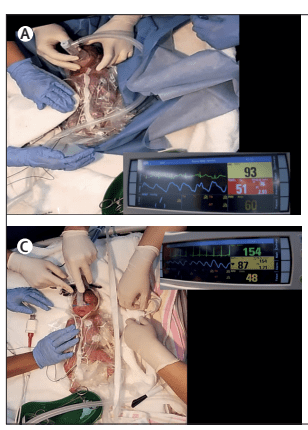
If the nasal CPAP was unsuccessful and the baby needed PPV, they were switched to a face mask. The authors supply some videos of the procedures, including this one of a baby started on nCPAP, then changed to face mask PPV.
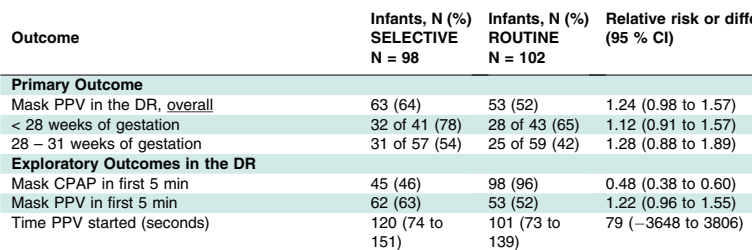
The primary outcome of the trial was CPAP success defined as the “proportion of infants managed with CPAP only (ie, without positive pressure ventilation, intubation, chest compressions or adrenaline) between birth and transfer to the NICU. If a newborn received no respiratory support, that was considered success of the treatment group.” The proportion of CPAP successes are shown in the following table.
All the usual clinical outcomes were similar between groups. Admission FiO2 was lower in the nasal group.
It looks like the advantage of nasal, compared to face mask, CPAP was because more of the face mask group required PPV, 47/77, compared to 31/74 nasal mask subjects. This is consistent with previous findings that face mask application can cause apnoea. Stimulation of the trigeminal nerve area can provoke respiratory pauses, and bradycardia, and it seems that the nasal mask, creating pressure over a much smaller area around the base of the nose, does not have this effect. The authors note that the starting pressure was intended to be 5 to 8 cmH2O in the 2 groups, but that the clinicians started the nasal CPAP at an average of 1 cmH2O higher in the nasal group. The nasal group also had heated humidified gases, compared to the cold dry gases in the face-mask group. These 2 differences are potential confounding reasons for the difference between the 2 groups. But, because fewer nasal group babies had PPV, the peak inspiratory pressure applied was lower in that group than the face mask group.
Despite these limitations, it seems that there may well be significant advantages in applying a nasal mask, compared to a face mask, for CPAP in the delivery room in the extremely preterm infant. Although the authors did not show any improvement in clinical outcomes (the study was not powered for such outcomes), any intervention which decreases the need for PPV during transition is probably a good thing for lung protection.
To put this in context of previous research, the Cochrane review, Ni Chathasaigh CM, et al. Nasal interfaces for neonatal resuscitation. Cochrane Database Syst Rev. 2023;10(10):CD009102, which did not include data from this trial, showed a reduction in the need for intubation in the DR with nasal interfaces compared to face mask. The 5 trials included in the Cochrane review were fairly heterogeneous: one included term infants; the nasal interface was a short nasal prong in 2 trials, short binasal prongs in 3 trials; and with a different device generating the pressure in the 2 groups in 2 of the trials. The Cochrane review showed a reduction in DR intubation, of note, this new trial had very few DR intubations, 6 in the nasal group and 7 in the face mask group; adding this to the Cochrane MA will have little impact, the weight will be small, and the tiny difference is in the same direction as the current MA results.
The review also showed less babies needing chest compressions, but that outcome was entirely dependent on the one trial that included full-term infants.
In the Donaldsson 2021 study the large majority of infants (<28 weeks) in both groups >82% received PPV. In Kamlin’s study, about the same proportion received non-intubated PPV (just over 50%) but fewer were intubated, McCarthy et al don’t seem to report how many infants needed PPV.
My interpretation of this is that it would be preferable in the very preterm infant to avoid face masks for initial CPAP support in the DR. It appears that the advantages of nasal prong systems and a nasal mask are similar, overall there is a reduction in the need for intubation in the DR, and perhaps for PPV.
This RCT from Colm O’Donnell’s group at the national maternity centre in Dublin enrolled 200 babies <32 weeks. The idea was to determine if there was an advantage to routine immediate CPAP application, using a round Fisher-Paykell face mask, cold dry gases, and a t-piece resuscitator. The comparison, selective, group had face mask CPAP (using the same system) applied if they developed signs of respiratory distress after 5 minutes of age. Infants in both groups had standard resuscitation, with PPV being started if they were apnoeic, or if they had a heart rate <100. The primary outcome was the requirement for PPV. Although the difference in the primary outcome was small and not statistically significant, more babies in the selective group required PPV in the DR, in both GA strata, and nearly half of the selective group received early CPAP (before 5 minutes).
More extensive resuscitation (intubation, chest compressions) was very similar between groups, as were all the clinical outcomes after NICU admission. Although the study did not show any differences that were “statistically significant”, there were no benefits to delaying CPAP.
My interpretation of all this is that the very immature infant would probably most benefit from early CPAP applied with a nasal interface. I like the idea of using a nasal mask to avoid the potential trauma of inserting a nasal prong; prong insertion can usually be done gently, but sometimes, especially in the smallest babies it is a tight fit and probably hurts. A really useful trial would be to investigate routine early CPAP with a nasal mask, which can also be used for PPV, compared to using a face mask according to current NRP standards.
I subscribe to Google alerts, which sends me an email whenever the phrase “neonatal research” appears on a new website or a new post. I was interested, therefore to receive an alert about an article which, according the blog “Bioengineer.org”, showed a major genetic contribution to the occurrence of Necrotising Enterocolitis.
The blog post includes the following quote “Bai et al.’s study represents a landmark in neonatal research by providing compelling evidence for the heritability of necrotizing enterocolitis in very preterm infants. The twin study design elegantly disentangles genetic predisposition from environmental influences and firmly establishes a genetic foundation for this complex disease”.
This was intriguing, so I checked on the original article. (Bai R, et al. Genetic susceptibility to necrotizing enterocolitis in very preterm infants: evidence from twin data. Pediatr Res. 2025). A nice study, from a group of authors in China, one of whom is my good friend Shoo Lee, working with the Chinese Neonatal Network. They collected data on NEC incidence and chorionicity of twin pairs of less than 32 weeks GA (or <1500g). They found no difference in the likelihood of a coherent diagnosis of NEC between monochorionic and dichorionic twins. They did further analysis restricting to surgical NEC, or comparing early and late onset NEC, and found no difference between mono- and di-chorionic twins.
In other words, the actual findings of the study are exactly the opposite of what the post on that blog stated. The conclusion of the Bai et al authors was : “heritability does not play a major role in the development of NEC”.
I don’t think an actual human being, reading the article, could possibly have misinterpreted the findings quite as dramatically as whatever generated the blog post. The post is accompanied by the following cute image, which they note was AI generated. My only explanation for this dramatic misinterpretation of the original research article is that the post itself is also AI generated, and that the AI engine just loaded the title and some sub-headings from the results (which are, indeed, misleadingly worded as if there were positive findings : “Heritability contributes to NEC” and “Heritability contributes to certain subgroups of NEC”), without being able to realize that the actual results show that the analysis, of what should have been sub-titled “Heritability contribution to NEC”, was actually zero.
At least this is on an obscure blog, and will probably not cause any harm. In contrast, actual primary publications are also being generated by AI, reporting research that never actually happened. Government policy is also being influenced by review articles written by AI, which include non-existent research, or research which has been misinterpreted, often purposefully so, for partisan ends. This is a major issue for the future of medical research.
Ybarra M, et al. Low-Grade Germinal Matrix Hemorrhage-Intraventricular Hemorrhage and Concomitant Preterm Brain Injuries: Neurodevelopmental Outcomes at 3 Years of Age. J Pediatr. 2025:114713. Previous studies of the long term outcome of infants with germinal matrix or low grade IVH have been inconsistent. Some have shown an association with poorer developmental progress, and others have shown no impact. Some of this variability may be due to uncertainty about diagnostic criteria, with slightly larger amounts of intraventricular blood being classified differently. Some is probably due to the variable association with other brain injury, not readily seen on ultrasound, such as white matter injury, or cerebellar haemorrhages. We now routinely perform imaging of the posterior fossa, which was not easy with older ultrasound machines, but small cerebellar haemorrhages are still hard to see, without MRI.
In this cohort from Toronto, 175 infants <32 weeks GA had ultrasounds, they also had early cerebral MRI at 32 to 34 weeks, if they were stable, and then again at term equivalent age. Neurologic and developmental assessments were performed at 3 years (Bayley version III). As for the results, low grade haemorrhages had no correlation with outcomes, unless associated with either large cerebellar haemorrhages or more extensive white matter injury. It has always been fascinating to me that germinal matrix haemorrhage, which destroys the primary source of cortical neurones, has so little impact on long term outcomes. It speaks to the plasticity of the newborn brain, if the Germinal Matrix is injured, other parts of the brain take over neurone production.
Take home message : there was no apparent impact of GMH or small intraventricular haemorrhages without dilatation on long term development. Cerebellar haemorrhages, if large, are associated with delayed language development at 3 years, and white matter abnormalities, if extensive, are associated with motor delay, and cerebral palsy.
Interesting review article on the impact of pasteurization, using the standard (Holder) pasteurization method, as well as some information about alternatives. The dash (-) in the figure above means no effect, rather than deletion. As you can see there are multiple impacts of pasteurization, as well as the expected impact on bacteria, some bacteria are resistant to Holder pasteurization, so donor breast milk still has an impact on the preterm intestinal microbiome. Both by direct colonization with the surviving organisms, but also because of the impact of HMOs and other components of human milk which remain despite pasteurization.
The figure also shows, in the upper right third, some alternative pasteurization methods which have been investigated, and which all show lesser impacts on breast milk components, HTST (high temperature short treatment) HPP (high pressure pasteurization) and UV-C (UV-C!). These alternative methods are equally effective at reducing bacterial load in the donor milk, and hopefully can be used in the future to give donor milk which is closer to Mothers Own Milk.
Take home message : Holder Pasteurization has major impacts on the composition of human milk. Alternative methods should be investigated, and approved.
In this observational study, the authors correlated the diet of a cohort of preterm infants <32 weeks GA with the findings on MRI at term. The cohort was enrolled over a long period, including a couple of years prior to the availability in their centre of donor milk (DHM) 2012-2014, and several years afterward 2014-2022. They include babies who almost exclusively received Mother’s own milk (MoM) and those receiving mostly formula, as well as the group with DHM. Brain volumes were greater in the human milk groups compared to formula, and diffusion tensor imaging showed diffusivity differences also, in the Corpus Callosum and the PLIC (posterior limb of the internal capsule). As the authors note, there is no good evidence from RCTs that DHM leads to better clinical neurological or developmental outcomes than formula. Nevertheless, these data are consistent with a beneficial effect of human milk on brain development, shared by DHM, and MoM.
Take home message : human milk seems to promote larger brains.
One of the benefits of MoM is that it routinely contains probiotic organisms, usually including Bifidobacteria. In this trial, 70 preterm infants <32 weeks were randomized to control or to a supplement of Bifidobacterium animalis susp lactis. As often happens in some journals the article is written in somewhat strange English; one example : “Quality control and data analysis were conducted after instrument analysis, using assessment of the peak significante equation of standard curves”. They ran a statistical comparison of the baseline characteristics of the randomized groups. This is a practice that Pediatric Research should know is ridiculous. If the groups were randomized, why run such a statistical test? It is superfluous, potentially misleading, and the CONSORT statement specifically states that it should not be done, Pediatric Research is supposed to follow CONSORT guidelines.
I started to include this article in the post as I thought it was a demonstration of the possible anti-inflammatory impact of this Bifidobacterium on the preterm intestine. But I now realize that I haven’t got a clue what most of it means. This following figure for example, is supposed to show correlations between a large number of “metabolites”; about 30 were selected from over 250 that were found in the stools, including, for example, 34 different bile acids. These figures are supposed to show correlations, negative and positive, between “metabolites”.
The legend to the figure states “Red indicates positive correlation, blue indicates negative correlation, and the darker the colour, the stronger the correlation. a Probiotic group week 2 VS Control group week 2. b Probiotic group week 2 VS Control group week 2″…. What on earth is this supposed to mean? Aside from the fact that the potential of at least 62,500 comparisons were possible, is this comparison within the 2 groups, or between the 2 groups?
What it seems to show is that they measured a huge number of molecules, the concentrations of some of them were correlated with the concentrations of others. But so what?
They also show dramatic differences in serum TLR4 concentrations between groups. I am unsure if circulating concentrations of TLR4 are of any interest; TLR4 is normally attached to granulocytes, as part of the receptor complex which recognizes lipopolysaccharide. Nevertheless, published serum concentrations range between the pg/mL range to the mg/mL range, with these new results being intermediate in the ng/mL range. Such enormously variant normal ranges (over 1 million fold differences) make me very sceptical about any results. Serum TNF-α and IL-Iß were also dramatically lower in the Bifido group. They also give exactly the same data, regarding clinical complications, in table 3 and a completely superfluous figure 10.
Pediatric Research used to be a journal that only published high-quality research, although they were rarely clinical studies, which was previously one of my criticisms of the journal. If this is typical of the quality of what is currently getting through peer review and editorial control, then the journal has fallen far indeed.
Take home message : Pediatric Research is no longer the high-quality source it once was.
This is a report of the 3 year outcomes of babies from a cluster RCT of a quality control initiative in Japan. The original publication showed no impact of the QI program (INTACT), so the authors combined the groups for this publication describing their neurological and developmental outcomes. Babies were VLBW and ranged from 22 to 31 weeks GA. Below is a selection from the extensive results, “severely delayed” refers to being <70 on the cognitive subscale of the Kyoto Scales of Psychological Development. The KSPD seems to have a similar mean to the BSID ver3, when tested on the same infants, but have a wider distribution, so a score <70 was considered severely delayed.
There was very little blindness or deafness, so, as usual, it was cognitive delay which was responsible for most of the infants who were classified as “NDI”. Unfortunately, the authors don’t report many things which matter to parents, in particular there is no mention of behavioural problems. They do have a table that they call “functional outcomes” but that is actually a report of the medical interventions being received by the infants, at 3 years of age, including home oxygen, NG tube feeding, anticonvulsant medications, etc. All of which were rare.
Take home message : The majority of survivors at every gestational age, even the most immature, do not have “moderate or severe NDI”. There is a progressive increase in “moderate or severe NDI” as GA decreases.