I received 2 comments about the last posting re: DCC. The way I set up this blog the comments aren’t necessarily very obvious, especially if you visit the home page rather than following a link to the individual posting. So I will sometimes copy parts of a comment into a new post. I will certainly never do that to criticize or embarrass anyone, just to try and further a discussion.
First a comment from Wally Carlo, who noted that Judith Mercer had an abstract at the PAS meeting reporting outcomes from a moderately large RCT of DCC. I didn’t put any data from that study in my analysis, because I don’t have the actual numbers, so I only put published articles in the Forest plots. But to clarify: Mercer’s study enrolled 208 babies under 32 weeks and basically showed no short term differences. The abstract doesn’t mention mortality, which makes me think that wasn’t significant either, but there were specifically no differences in IVH, or sepsis.
The other comment was from Michael Hewson, and I quote some of it here
It could be getting difficult to continue with the APTS trial enrollment after explaining to parents that in the data available so far delayed cord clamping reduced mortality and NEC by at least 50% (admittedly there is a 2.5% chance of obtaining such dramatic benefits by chance alone). It’s true that more data would be great, that we don’t have enough long term outcome data, and that APTS could theoretically swing the pendulum in the other direction (like INIS or BOOST) but still how to look past the existing delayed cord clamping data, including the physiological evidence?
There seems to be a tricky no mans land that is reached after the point of equipoise has been passed but before widespread acceptance of a new intervention… therapeutic hypothermia also springs to mind.
I think those are important points, both the specific point about this issue, and a general point about how much evidence is enough.
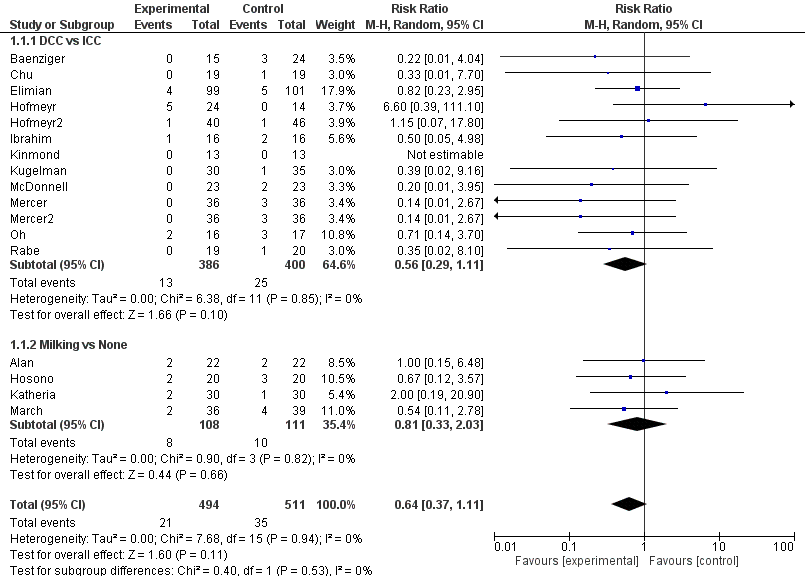
The summary statistics of the data that I selected for my Forest plots (I must emphasize that this is not an ‘updated systematic review and meta-analysis’ it is me trying to summarize what I think are the relevant data), show a difference in mortality which is actually between 6.8% in controls and 4.3 % with DCC. That makes the risk difference 0.025, with an NNT of 40, 95% CI of 20 to infinity. The p-value for the mortality difference is 0.11, which is not a 2.5% likelihood of being due to chance.
For trainees and others everywhere, what this p-value means is that random selection of 2 groups of patients from the population of very preterm infants would show differences as great, or more extreme, 11 times out of 100.
Now I don’t think that’s enough to be sure that this procedure is safe, let alone advantageous. I think it is probably safe, the likelihood of significant harm seems quite low from the data that have been collected so far.
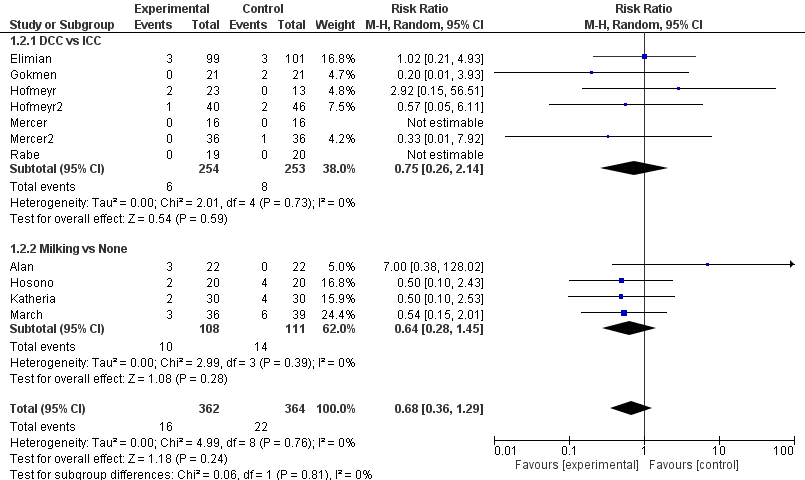
The difference in NEC is 7.4% in the controls, and 3.8% with DCC, among the studies that reported the outcome, there were many studies that did not report NEC, so there are only 30 events in total, among over 500 babies in the trials with this result. But if we assume that those that didn’t report NEC did not have any (which is a dangerous assumption, but many of those trials were larger babies who were at lower risk), then the difference is between, 3.9% and 2.0%, or a risk difference of 0.019, and an NNT of 52, 95% CI also include infinity!
The p value for the difference, using the trials that reported NEC which I put in the meta-analysis, is 0.09, far from what we usually consider to be significant, and again not a 2.5% likelihood of being due to chance, but much more than that.
If someone was to do a Jesper Brok style sequential analysis (Brok J, et al. Apparently conclusive meta-analyses may be inconclusive—Trial sequential analysis adjustment of random error risk due to repetitive testing of accumulating data in apparently conclusive neonatal meta-analyses. International Journal of Epidemiology. 2009;38(1):287-98.
which I have neither the time, the expertise, nor the software to do), I can bet you that it would be far, far away from a significant result.
We’ve been here before, as is mentioned in this comment, based on multiple small studies, IVIG seemed to reduce mortality in septic newborns. INIS showed absolutely zilch. Fortunately there was no prior evidence of harm in the IVIG studies before INIS, and that trial also confirmed that there was no harm.
I appreciate the comment about the importance of making sure parents are well informed of the current state of the literature when getting consent to enroll them, that is of course essential, and these things can be difficult to explain, but I would insist that it is by no means clear that the differences in mortality or NEC are really due to the DCC. Hopefully enough parents will agree that this is an important question to answer, and will consent to randomization. I think if a parent, presented with this information, requested DCC (or requested immediate clamping) there would be no good reason for denying it. If you are set up to do the study then presumably you have equipoise, so organising a DCC should be no problem.
As there is no “trend” towards harm in any of the outcomes presented, and babies who have DCC need less blood in most of the studies (but interestingly not in that study by Judith Mercer, the hematocrits, at least, were no different between groups) I think it is unlikely that we are harming babies with DCC, but there really isn’t yet any reliable evidence of any benefit other than a possible reduction in blood transfusion. Most of that data of course comes from more mature preterm babies; for us to ensure that this is really safe, and that there are real benefits for small preterm infants, requires us to finish large studies if we at all can.
I think the example of the hypothermia studies is not a clear parallel. It became difficult to randomize after the publication of two large high quality multicenter trials, after the 3rd was published I was of the opinion that the other studies should stop, and that it was no longer appropriate to continue to randomize patients. We are far from that situation with DCC in the very preterm baby. Even one well done, large multicenter trial, if it showed no harm, and clarified what the real benefits might be, could be enough to appropriately change practice everywhere.