
The multicentre project, that I started the last post with, has just published a new important article, which addresses the duration of antibiotic treatment (Dimopoulou V, et al. Antibiotic exposure for culture-negative early-onset sepsis in late-preterm and term newborns: an international study. Pediatr Res. 2024) and is particularly focused on those babies with negative blood and/or CSF cultures. They divided the babies who received antibiotics without ever having a positive culture into those which were treated for less than 5 days, or for at least 5 days.
I think that 4 days of treatment, for a well baby with risk factors who has negative cultures, is already far too long, the optimal duration for such a baby would be 0 days! But, given that there was enough concern to perform a blood culture, then antibiotics can be stopped after 36 hours, with only a tiny possibility that a true-positive blood culture will become positive after 48 hours, and then very rarely for organisms treated with our usual empiric antibiotics.
But what about those babies who are thought to have “culture-negative sepsis”? In this new study, babies treated with antibiotics for 5 days or more, one extant definition among many, were 20 times more frequent than true EOS. There were 8000 babies with negative cultures who received treatment for >4 days, compared to 375 with a proven EOS.
What are we treating, when we continue antibiotics despite negative cultures? I well remember some twins (more than 1 pair) where one twin was sick with sepsis and positive cultures, and the other was similarly sick, but with negative cultures. To me, those cases have been the best proof that culture-negative sepsis does indeed exist. But what is it? Many such infants do not have an active bacterial infection. Many have circulatory and respiratory illness caused by the inflammatory cascade following a bacterial infection. Some cytokines have been shown to cross the placenta, such as IL6, for example, so the infant could become passively ill as a result. In other cases the infection may already have been effectively treated, such as when a mother had chorioamnionitis, and has received antibiotics. In such a case the infant is affected by the cytokines and other inflammatory mediators released by the mother or by the infant themselves. In the example I gave at the beginning of this paragraph it may be that a truly infected co-twin sets up enough of an inflammatory response that their sibling is symptomatic.
In such an infant, blood cultures will be negative, but also they will not benefit from antibiotics. The sensitivity of current culture techniques are such that, down to about 1 CFU/m, over 98% of cultures are positive, and any concentration of bugs higher than this will rapidly make the culture machine alarm ring.
For a more complete discussion of the issues in “culture-negative sepsis” you could do no better than to read Joseph Cantey’s article from the Journal of Pediatrics in 2022. I can’t tell if it is open access, but if you have difficulty getting it, I am sure we could find a way to get a copy to you.
I mentioned, in the part 1 post, another recent publication, with probably some overlap in the data, from a national Swedish database (Gyllensvard J, et al. Antibiotic Use in Late Preterm and Full-Term Newborns. JAMA Netw Open. 2024;7(3):e243362). In that publication the incidence of EOS had fallen over time up to 2020, and treatment of culture negative infants had decreased also, but the gap had actually widened. Also, in that study, the median duration of antibiotic treatment among all infants with negative cultures was 5 days, IQR 3-8 d, 97% of infants who received antibiotics had negative cultures. It is clear that not all infants who have a culture taken and are started on antibiotics have sepsis, culture-positive or -negative. Although there do not appear to be national Swedish guidelines for when to screen for and treat neonatal sepsis, there are guidelines about when to stop them (again translated by Microsoft Word)
Full-term child with suspected early onset sepsis (illness before 72h): discontinue antibiotics after 48-72h and do not diagnose as neonatal infection:
• Never required ventilator care or had septic shock
• Mother not diagnosed with obstetric infection
• Blood culture negative, growth of contamination or not yet responded to
• Well-being at 48-72h age
• CRP peaks below 60 mg/L, and CRP decreases during antibiotic withdrawal
• CRP peak between 60-100 mg/L, and CRP in decreasing consider discontinuing antibiotics
The way I understand it, you need all of those in order to stop the antibiotics; thus, ongoing treatment of increased CRP concentration without other signs of infection is recommended by this guide, a practice which has no evidence-base, and leads to major over-treatment of uninfected babies. Previous publications have shown that you can stop measuring CRP, and routine CBCs, without any adverse impact, only a reduction in unnecessary antibiotics. Although the Swedes are doing much better than most of us in reducing the number of antibiotic courses administered, they are still treating 50 babies with antibiotics for every truly infected infant, and as noted, they treat for a median of 5 days. If they just stopped doing CRPs, but still used the other criteria in that national standard, they could do even better, and there is no evidence that there would be any risk involved. It is well known that CRP concentrations increase several hours after the initiation of inflammation, so they are usually ignored if they are low during the initial sepsis evaluation. They also increase easily and are very non-specific, so they should also be ignored in later analysis of whether an infant has “culture-negative sepsis” or not.
There has been a lot of woolly thinking about this. Infants are defined as having “culture-negative sepsis” if they are treated with 5 days or more of antibiotics. Studies have then shown that infants with “culture-negative sepsis” have higher CRP concentrations, and this is published as evidence that CRP concentrations are useful in the diagnosis of the phenomenon. But, it is often the high CRP which leads to the prolonged antibiotic use. Circular reasoning anyone?
One early study of the neonatal use of CRP, for example, showed that 9% of the babies who were considered “definitely not infected” had raised CRP. Infants delivered vaginally have higher CRP than those delivered by Cesarean, especially CS without labour. Infants with a final diagnosis of TTN have higher CRP, as do those with Meconium Aspiration, who are often treated with prolonged antibiotics in the absence of other risk factors for sepsis. In part, this is probably because CRP increases to a mean of over 40 at 48 h in such babies, despite negative cultures and no evidence of any benefit from antibiotic use.
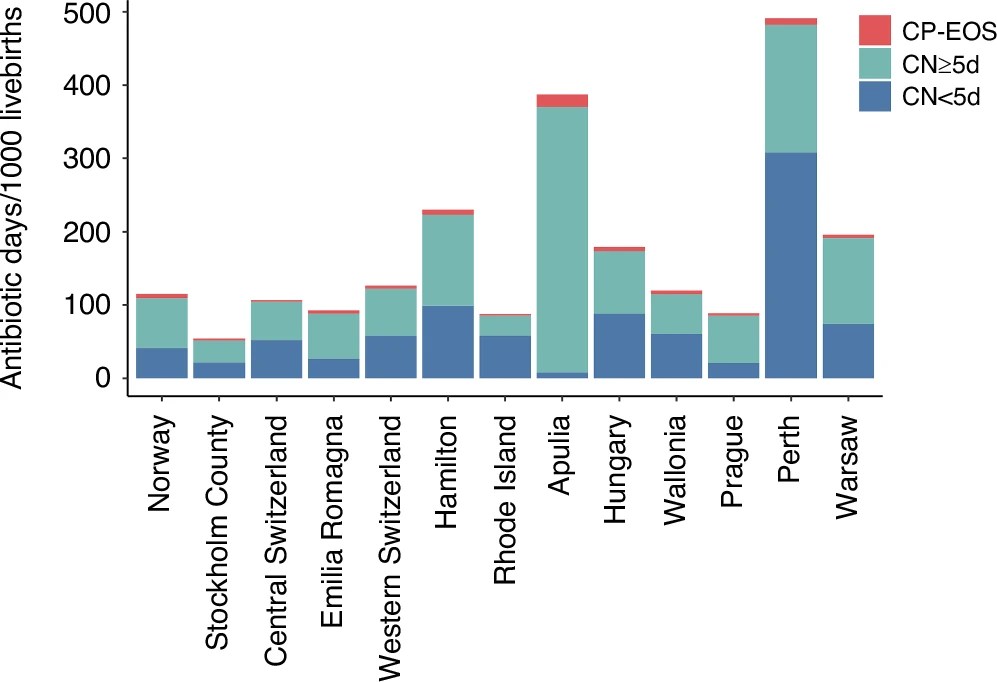
As this figure from the new article shows, the babies who clearly do need antibiotics, in red, are vastly outnumbered by the others, both the group with <5 days antibiotics, and those with 5 or more days. And there is enormous variation between networks.
Routine stopping orders for antibiotics after 36 hours, and requiring a conscious decision to continue if cultures are negative, could immediately have a big impact on exposure. A re-evaluation of each case, and a thoughtful answer to the questions “does this baby really have “culture-negative” sepsis?” and, “is this baby likely to benefit from continued antibiotic therapy?”, which are linked but not identical questions, could further reduce the unnecessary overuse of antibiotics. It would help to preserve their usefulness for the future, as well as reducing adverse impacts on that individual.







Thanks Keith.
This is a subject that is increasingly dear to my heart. In the NICU I work in, ~50% of infants >=35 weeks admitted in the first 2 days receive antibiotics. Thankfully most finish after 36-48 hours, but the vast majority of them did not need them to start with. There is a fear of sepsis that influences a lot of decisions.
Around 35% of our term babies with TTN following a planned LSCS not in labour with intact membranes receive antibiotics. If they have a positive culture, it is always a contaminant. Which results in another culture, and a more prolonged course of antibiotics.
We have to start looking at what we are doing to this group of babies and rationalise our antibiotic use in very low risk populations.
And don’t get me started on the CRaP test…
Where I work those babies (planned LSCS not in labour) rarely get antibiotics, but some of them still do, even though the risk of infection is ZERO. Some of my colleagues, especially the more junior find it difficult to not give antibiotics, even for iatrogenic HMD after a planned CS. We still have work to do, to define those babies that can safely not be treated, and instill that into daily practice.
This article complement the previous about be carefully at time to indicate antibiotic treatments and suspend it if there no positive culture or sepsis clinical scenario, and continue examination after your decide stop antibiotics. The Joseph Cantey’s is open access thanks