
Recent publications about platelet transfusions in the newborn.
Hopefully, everyone has integrated the findings of Planet-2 into their protocols and guidelines. Curley A, et al. Randomized Trial of Platelet-Transfusion Thresholds in Neonates. N Engl J Med. 2019;380(3):242-51. This trial, in preterm newborns <34 weeks with any cause of thrombocytopaenia, apart from those with a recent major bleed, showed that a transfusion threshold of 25,000 led to fewer complications, including less bleeding, than transfusion at a more liberal threshold, of 50,000. The trial excluded babies who had a pre-existing “major IVH” which was defined by an intraventricular bleed with dilatation, or an intraparenchymal bleed of more than 2 cm maximum diameter on an ultrasound taken within 6 hours of randomization.
A publication from our NICU (Zabeida A, et al. Platelet transfusion practice pattern before and after implementation of a local restrictive transfusion protocol in a neonatal intensive care unit. Transfusion. 2023;63(1):134-42) showed that our new guidelines, which mimicked the entry criteria for Planet-2, decreased the proportion of babies getting platelet transfusions, among all NICU admissions, from 9% to 5%, and eliminated the small number of babies who had previously sometimes received more than 3 transfusions. We were able to abide by the protocol for 70% of the transfusions, with some of the 20 transfused babies receiving transfusions at higher threshold because of active NEC, or being acutely postop. Three babies received transfusions because of low platelet counts (above the threshold) after ibuprofen treatment, and the concern that the ibuprofen causes platelet dysfunction, and there were 3 other protocol “violations” for different reasons.
Another publication, this time from Bob Christensen’s group, (Bahr TM, et al. Platelet Transfusions in a Multi-Neonatal Intensive Care Unit Health Care Organization Before and After Publication of the PlaNeT-2 Clinical Trial. J Pediatr. 2023;257:113388) did not show a reduction in the proportion of babies receiving a platelet transfusion; 2/3 of the transfusions in their study, even after the guideline change, were given with platelet counts above 25,000. They did have some minor trends to reduced utilisation of platelets, (13 babies transfused per 1000 admissions compared to 16 before) but not what they were expecting.
These are the guidelines before and after the change

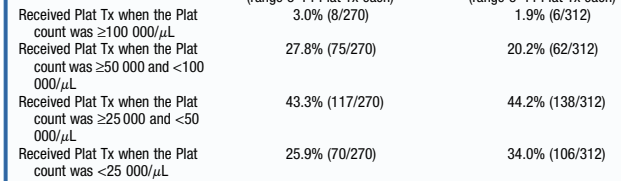
As you can see in this extract from their results table, most transfusions were still being given above 25,000
Another study, from a couple of years ago, also studied platelet transfusion before and after a more restrictive guideline, that guideline also has a threshold of 50,000 for infants considered to be at risk of IVH, (<28 weeks and <7 days). In contrast to the above study, they showed a dramatic reduction in platelet transfusions, from 25 per 100 admissions to 12. (Davenport PE, et al. Implementation of a neonatal platelet transfusion guideline to reduce non-indicated transfusions using a quality improvement framework. J Perinatol. 2021;41(6):1487-94), few of which were outside of their new guidelines. The justification given for the higher threshold in their guideline among infants at risk of IVH was “since the average time of randomization in the trial was day of life 7, and 39% of infants received a platelet transfusion prior to randomization, it was possible that these transfusions were given during the highest risk period for ICH”.
Long term follow up of the babies in the Planet-2 trial (Moore CM, et al. Two-year outcomes following a randomised platelet transfusion trial in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2023;108(5):452-7) has now been published. The original publication reported death up to 28 days, but as far as I can see, nowhere does it report the total number of survivors per group, which should be mandatory, surely, for any RCT. The best I can find is a table in the supplemental materials, that shows the number of deaths which followed a Serious Adverse Event was 52 in the restricted, and 58 in the liberal transfusion group. In the 2 year follow up, the mortality before 2 years was 70 vs 91 (<25,000 threshold group vs <50,000 group), so there were either a lot of deaths after discharge, or a lot of deaths that were not considered a serious adverse event!!!
Among the survivors, there were a few more adverse outcomes for each outcome in the higher transfusion threshold group. There were 13% with CP compared to 10%, and slightly more with blindness, deafness, and seizure disorder. An important outcome which they reported was called “global developmental delay”, this was assessed variously, sometimes by formal testing, but often by an informal assessment conducted by a health care professional, who found the infant to be more than 9 months delayed in their development. I am very unsure how reliable this is as a method for determining “global developmental delay”, but I don’t think there is a good reason to suppose that the reliability would differ between groups; 44% vs 33% were given this appellation, with, again, the liberal, higher threshold, transfusion group being worse off.
There were also many more infants on oxygen (or respiratory support) at 2 years of age from the liberal transfusion group, 11% vs 4%. This is pretty serious lung injury, with more than twice as many infants being affected in the higher threshold group.
Given all of these adverse outcomes in the higher threshold transfusion group, and the lack of acute clinical benefit, you really need a good justification for transfusing above 25,000. It often takes a while to change clinical practice, and there may be occasional reasonable indications for transfusing earlier. Evidence-based protocols almost always improve practice and outcomes, they should be applied thoughtfully, and the impacts evaluated in day-to-day practice.
Given the lack of any benefit, and the higher risk of bleeding, with earlier platelet transfusions, and the concern that the results may not be applicable to babies at highest risk of IVH, or at-risk of extension of a previous major IVH, we need more trials. A trial that enrolled babies at birth, and/or which included babies with pre-existing severe intracranial haemorrhage, and/or examined even lower thresholds, would be feasible, and I think acceptable to many. One day we will know when to transfuse platelets, on this planet!







Great overview, thank you for writing and sharing. I couldn’t agree more with your recommendation to be restrictive with the use of platelet transfusions.
Unfortunately, we showed in a recent survey in Europe, and US colleagues found similar data in an observational study, that a substantial proportion of NICU’s still uses thresholds above 25.(https://fn.bmj.com/content/108/4/360.long, https://pubmed.ncbi.nlm.nih.gov/33836184/) We hope to generate more data to understand the reasons behind this variation. And given that at least part of it is probably due to lack of implementation of the trial results, we may need continued effort and implementation projects to improve this. A secondary analysis of the original trial has helped convince some to change practice, which might be relevant to mention here.(https://doi.org/10.1182/blood.2019000899)
Ultimately, I would be most interested in a trial which allows us to ‘search’ for the optimal thresholds, for example via an adaptive trial design. And preferably a trial which looks at more than just platelet count as a transfusion indication, since we know that the association between the severity of thrombocytopenia and bleeding risk is not clear. And lastly, I think key before moving on to a next trial is that we have a better understanding of the pathophysiologic mechanisms that lead platelet transfusion related harm, through basic/preclinical/translational research. Not many people focus on this topic, but some important work is being done.(eg https://www.sciencedirect.com/science/article/pii/S0006497121041045)
In short, lots to do, but a restrictive transfusion strategy is probably our best bet for now.
Thanks for the comment, there are indeed many unanswered questions, Planet-2 only enrolled preterm infants, hypothermia treatment seems to have dramatic effects on platelet function, does that mean we should transfuse at a higher threshold? Perhaps the transfused platelets are even more dangerous in this situation, and we should transfuse at lower thresholds.
Just like our babies who had transfusion of platelets above our current threshold after ibuprofen treatment, that may be the right or wrong thing to do.
I agree that the bleeding risk probably differs by cause of thrombocytopaenia, if I remember right the incidence of bleeding with alloimmune thrombocytopenia and immune thrombocytopaenia secondary to maternal ITP are quite different, and lower in ITP, but doing a quick search I actually can’t find good data to confirm that memory, just repeated references to older literature!
The harmful effects of platelet transfusion certainly require more investigation, although proinflammatory effects are clear, that doesn’t explain to me why bleeding is more frequent.
I think a really urgent question is what level to transfuse prior to surgery. Not at all uncommon to have throbocytopaenic babies who need surgery, and we may be increasing their risks by transfusing at higher thresholds.