
Hernia repair timing
One trial which will should have an impact on the care of newborn infants is the trial of early versus late hernia repair. 40 neonatal centres in the USA randomized 320 preterm infants to inguinal hernia repair before discharge (between 37 and 42 weeks, if I remember correctly) or later repair after 55 weeks PMA (55-60 weeks according to the record on clinicaltrials.gov). That record also notes a sample size of 600, and notes that a Bayesian analysis of the data will be the primary method. The primary outcome was a composite of adverse events, which I can’t now find details for but included things like post-operative apnea, requiring intubation post-op, and incarceration of the hernia.
The justification for pre-discharge repair has always been that incarceration was relatively common, and we should repair the hernia before discharge so that doesn’t happen. Incarceration did occur in 4.5% of the late repair group, it was defined as needing surgery, sedatives or a surgeon to reduce the hernia. There were a few incarcerations in the early treatment group as well.
Overall there were more adverse events in the early surgery group, 26%, than the late group, 18%, which made it highly likely (96% probability) that late surgery led to fewer adverse events. The total number of hospital days after randomization was also shorter in the late repair group. One somewhat unexpected finding was that 10% of the hernias resolved in the late group. Apparently this has been suggested before (many years ago), and was probably a real finding, as the presence of most of the hernias was confirmed independently.
Some of our families live hundreds or thousands of kilometres away, and re-admission for later hernia repair may be more of a problem for them. But for the majority of families who live with easy reach of my hospital, it looks like we should probably wait for 3 months post-discharge before fixing their hernias.
The only real disappointment of this trial is the lack of a catchy acronym, it could have been HIDE (Hernias of the Inguinal region, Delayed vs Early repair) or some combination of S (for surgery) HI and T (for trial)…
Premies are cool enough
A randomized trial of cooling for asphyxiated preterm infants who have not been well studied in previous trials (33 to 35 weeks gestation) but who sometimes get cooled, because of “mission creep”, was performed by the NICHD network.
The calculation of sample size was interesting, as they designed the trial to get the largest sample which they considered feasible within a reasonable time, and planned a Bayesian analysis of the trial. They planned to enrol 168 babies, and achieved that, and care was identical to that for more mature babies, with careful normothermia in the controls, and 33.5 degree target temperature in the hypothermia group. Cooled babies were more likely to become hypoglycaemic, and more likely to have major bleeding, but most importantly more likely to die, 21% vs 15% with a Bayesian calculation of a 77% probability of a real increase in mortality with cooling compared to normothermia.
The primary outcome was death or “disability”, which was a Bayley 3 cognitive score <85 or GMFCS >2 or a seizure disorder or deafness. The primary outcome was very similar between groups, with a neutral probability on Bayesian analysis of being better or worse.
This is probably the best evidence we will get for the efficacity of therapeutic hypothermia in late preterm infants, and strongly suggests that it is not effective, and may be harmful.
Mild HIE, to cool or not to cool, that is the question.
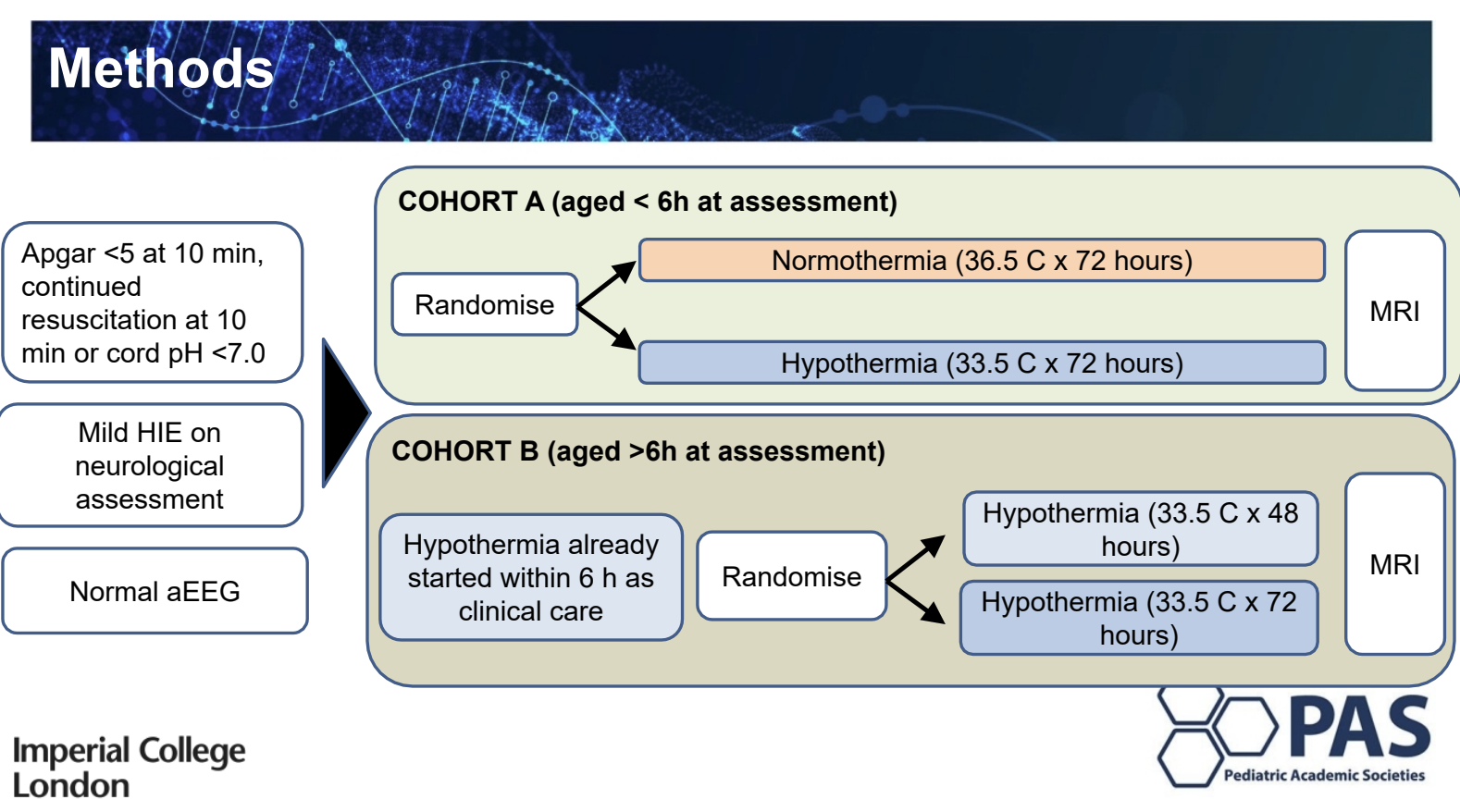
From Imperial College London a combined report of 2 trials targeting term babies with signs of mild encephalopathy. They had to have a clinical examination, in the mild category, and a normal aEEG. The trials includedonewith babies randomized before 6 hours, who were then treated with normothermia or standard hypothermia, and a second group of babies who were already cooled, and who were >6 hours of age, they were randomized to shorter or standard hypothermia.
The trials are quite small, and so far only short term outcomes and MRI were available. Cooled babies were more likely to be intubated and to need inotropes. They also had longer hospital stays. As for the MRI results, they appear to be worse in the cooled groups than the normothermic infants.
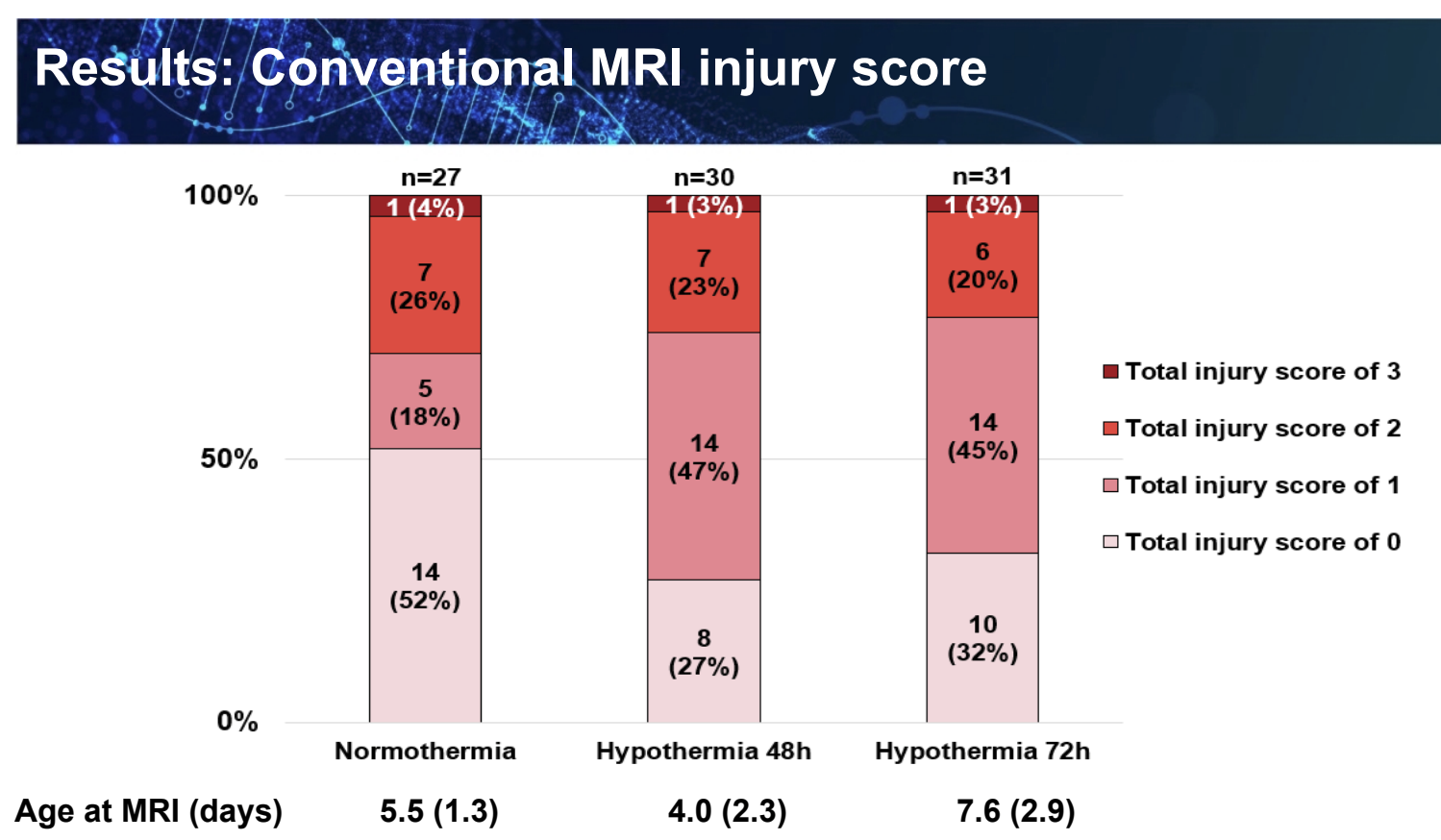
As I wrote previously MRIs are very poorly predictive of outcomes on an individual basis, but there are overall correlations in groups of babies between poorer outcomes and worse MRI scores.
Therapeutic hypothermia for mild HIE has been growing in frequency, and I have been guilty of starting it when I wasn’t sure whether to, or not. I felt from previous data that it was probably safe, and possibly effective. I may have to revise that opinion, but clinical examination may change prior to the time limit for cooling, and babies with normal or mild encephalopathy may deteriorate. I think based on this data that we should be cautious cooling babies who are clinically in the mild category, ensure that they are re-examined at 5.5 hours and have aEEG or EEG. If the examination only shows signs of mild encephalopathy, and the electricity is normal, then scrupulous maintenance of normothermia and supportive care is indicated.







Thanks for the precise and timely summary
The hernia repair trial did have a catchy “hip” acronym…It was “HIP” (https://med.uth.edu/pediatricsurgery/hip-trial/)