
Previous randomized trials of routine cerebral NIRS in preterm infants have shown that cerebral hypoxia can be reduced by responding to the signal, but in an underpowered follow up of a subgroup, there was no impact on long term outcomes. The same investigators, in an expanded collaborative of 70 NICUs studied the impact of routine monitoring of cerebral oxygenation on brain injury as shown on ultrasound up to 36 weeks PMA. Hansen ML, Pellicer A, Hyttel-Sorensen S, Ergenekon E, Szczapa T, Hagmann C, et al. Cerebral Oximetry Monitoring in Extremely Preterm Infants. New England Journal of Medicine. 2023;388(16):1501-11.
The definition of the outcome was “one or more of: intraventricular hemorrhage of grade 3 or 4, cystic periventricular leukomalacia, post-hemorrhagic ventricular dilatation, cerebellar hemorrhage, and cerebral atrophy” which are all defined more precisely in the supplemental material. One quibble I have with the definitions is of grade 4 IVH, defined as “parenchymal haemorrhagic infarction visible in the periventricular white matter”, what we actually see is echodensity, and it is not possible to really ascribe a mechanism of injury to an ultrasound appearance. As an upcoming review article that I co-authored will point out, periventricular echodenisities are not all strongly associated with poor long term outcomes. The extent, location and whether uni- or bi-lateral are all important.
This study was large enough (n=1600) to show moderately large differences in the incidence of ultrasound abnormalities, 90% power to show a reduction from 34 to 26% among infants <28 weeks GA. Monitoring had to start within 6 hours of birth and continue for 72 hours, a treatment algorithm was followed to protocolise responses to low cerebral saturations.
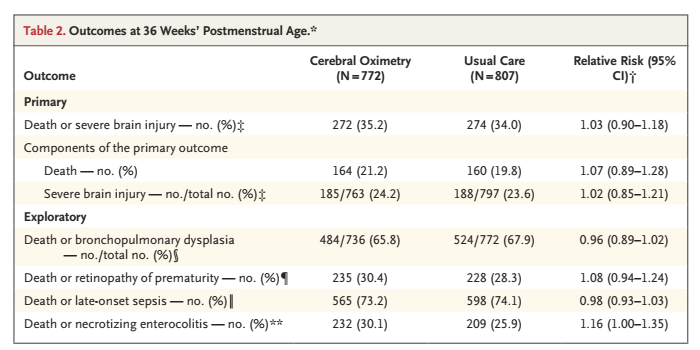
The results in the 2 groups were, basically, identical.
My big question is whether this is a surprise, I think that low cerebral oxygen saturations are due to a large number of different processes, and that there is not a clear link between low cerebral oxygen saturation and severe IVH or PVL. Only 29% of the babies in the oximetry group had a change in management because of low saturations, so you would only expect the intervention to have any impact on that 1/3 of the babies. PVL may occur after an episode of shock, but the strongest correlation is with perinatal inflammatory disorders, like chorioamnionitis.
I also think it is a real possibility that less cerebral hypoxia could improve long term outcomes without necessarily changing brain ultrasound findings, and I really hope that after this great effort to perform a really important trial, there will be long term follow up of the survivors.
For now there is no clear evidence that routine cerebral NIRS, and responding to low cerebral oxygenation, improves short or long term clinical outcomes in the preterm.






